This piece by The Auricle‘s Co-Editor, Lachlan Coman, dives into the fascinating world of medicine at high altitude. It first featured in The Auricle‘s October-December Edition in 2022.

This piece by The Auricle‘s Co-Editor, Lachlan Coman, dives into the fascinating world of medicine at high altitude. It first featured in The Auricle‘s October-December Edition in 2022.

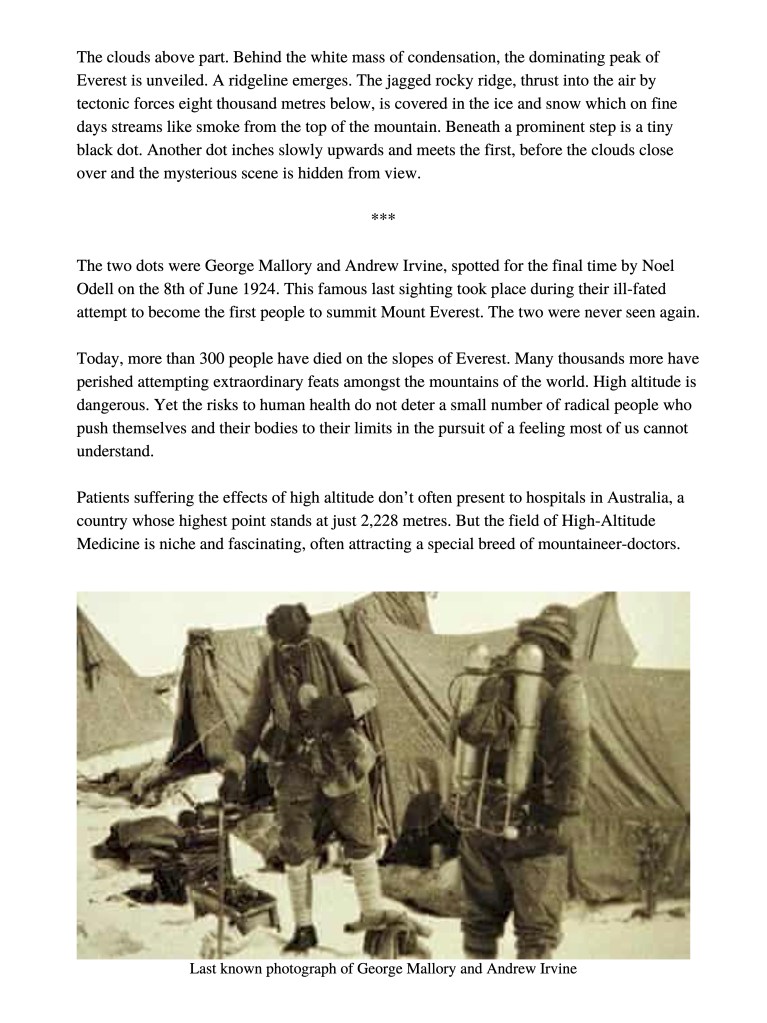
This writing was submitted by Jarrett Lee, a Year 2 Monash medicine student, and was first published in The Auricle‘s October-December Edition in 2022.
Human beings are fragile. We cut ourselves while preparing dinner, fracture our limbs playing a game of footy, and damage our organs with a tad too many beers. Medicine, however, never fails to offer a way out on every occasion. We have our wounds stitched. Our bones fixed. Our livers changed. But when confined within the parameters of what medicine is capable of, and confronted with the realities of decline and mortality, we as fragile creatures are often left unready and unprepared. It is often acknowledged that the duty of a physician, in its empirical form, is to fix. We pride ourselves on our ability to repair, to mend and to recover what is broken. But when we encounter a disease that cannot be treated, or a wound that is unable to close, when we as physicians are challenged with a problem that is no longer fixable, herein lies the moral conundrum. Do we forge ahead, knowing that medicine can possibly do more harm than good? Or can we muster up the courage to recognize the finitude of our lives, and accept the painful truth that we are in fact – dying?
As I foray through my last semester of pre clinicals, I grapple with this dissonance – the jarring disconnect between the principles of what medicine can accomplish, and its otherwise obvious reality. And strangely enough, the struggle to understand the inevitability of death and dying, albeit a grim one, has framed carefully my beliefs on what medicine truly sets out to do, and forged, in the crucible of mortality, the cornerstone upon which my beliefs as a doctor-to-be, have been built. Yet above everything, there remains the question,heavy but eloquent, one written so beautifully by Paul Kalanithi in his novel ‘When Breath becomes Air’. A question that seems to shoulder the weight of mortality, yet beautifully encapsulates the soft fragility of human life. And so, I ask – ‘what makes life meaningful enough to go on living?’
In the years to come, I hope to become a doctor, one who can answer this question with much confidence. A doctor brave enough to understand when to recognize defeat, and when to keep on fighting. One who isn’t afraid of telling a young mother that the cancer has spread to her liver, her brain, her lungs and her bones; and that she is almost certainly going to die. A doctor willing to lay down hard truths; that it might betime for her to halt the drugs and the surgery, and instead consider what might truly be important – spending time with her family.
In the years to come, I hope to become a doctor, not one who understands death, but one who understands what comes directly before. A doctor who understands that human beings do not fear dying itself, but the process of dying, the process of losing the very qualities that make us Human. And when that defining moment begins to bare its fangs, I can only hope to be the doctor who dulls the teeth of mortality, so death becomes just a little less – harrowing.

This writing by Charlie Ho from MUMUS Community and Wellbeing, first published in The Auricle‘s Final 2022 Edition describes the weight of external and internal pressure, and how to break free from its constraints.
Mediocrity, such a word reminded me of a bland taste, a lukewarm sensation, an apathetic aloofness. It had evoked in me dissatisfaction, disappointment, even disdain. After all, mediocrity must have resulted from a callousness, an insincerity, negligence of duty. Mediocrity means that I hadn’t worked hard enough or done my best; it was glaring evidence of my mistakes, yet another blemish painted on the proof of what a failure I was. I sighed, then scoffed at myself thinking about the things I could have done differently, a wave of “what-if”s flooding my head. After all, a mediocre result isn’t exactly going to get me anywhere. After all, my best was never good enough. Who cares about my efforts when outcomes are all that matters? I released my breath I had been unconsciously holding. I took a final glance at the report in my hands and tucked it away into the depths of my bag, as it by removing from sight the document would lessen the pang of guilt I felt being branded as mediocre.
That pretty much sums up what used to be my train of thought every time I checked my score and feedback for any assessment. I’m sure it is not an unfamiliar experience among us medical students, given the tendency of doctors being perfectionists. Yet, over time, I have come to peace with mediocrity and learnt to embrace and appreciate the feeling.
Born into the cut-throat culture of Hong Kong, I had been conditioned into viewing life as a race. The real pressure of getting a head start early on in the race was plain as day — parents filling up their children’s timetables with endless classes, extra curricular activities and competitions from the moment they speak their first word, devising a strategy for getting into a “Band 1” secondary school, camping overnight just to be first in queue for a chance of their kid getting in a prestigious kindergarten. Instilled in me was the doctrine that being mediocre was to be left behind, a loser deserving of none other but the worst. Mediocrity was simply not an option, god forbid even mention burning out — if I couldn’t handle a little stress, I must be weak-willed and unworthy of anything.
Of course, that sort of mentality only proved to be detrimental to be mental wellbeing and soon, other areas of my life started to be affected as well — my hobbies, sleep, physical health, relationships — it seemed as if my life had become undone by my own hands, the roots of despair digging deeper and deeper down my mind. All the self loathing begot worse performance which continued the vicious cycle and before long, I hit rock bottom.
Fortunately, you being able to read this piece means that I have gotten better and here is something I wish I could have told myself about mediocrity earlier on.
First is arguably the hardest step. Accept mediocrity and the discomfort that comes with it. Be compassionate to yourself when you don’t meet your own standards. Getting muddled in your head about how terrible it is that you have done a mediocre job is going to be harmful at best and will definitely not help in any way whatsoever. Know that recognising the mediocrity is proof that you care about what you do and is the first step towards improving your craft. It is in fact possible to be your own critic while being kind to yourself.
Next is something easier said than done. Enjoy the process leading up to the end result. If what matters are only results, your motivations may not be the most sustainable and you might consider rethinking your reasons for doing that something, perhaps even consider taking a break and coming back to see if that something is what you truly want to do. Once you start enjoying the process, the end result typically tends to turn out better, while a mediocre result ends up not having that much of an impact on your overall wellbeing, overall increasing your capability in producing a better result.
Last but not least may be the cheesiest advice I’d give myself: even if you never end up with something that exceeds mediocrity, you are and will always be good enough.

This piece by Laura Gilbertson, from MUMUS Community and Wellbeing, describes the feeling of leaving medical school, and the new horizons that emerge. This piece featured in The Auricle‘s October-December Edition in 2022.
With the end of medical school fast approaching (for some of us at least), I thought I’d check in with some of the things I’m feeling as this phase of life comes to a close.
Change is incredibly scary. It’s certainly not easy saying goodbye. Goodbye to friends, to places, to teachers, to memories. Goodbye to being a student, the world of no responsibility and of clocking off at lunch time.
And yet at the same time there is the excitement of something fresh. The world of work. The possibility of new friends and new memories. That feeling you get when you hold the pager or make a referral (and only get yelled at a couple of times) – like, hey, maybe I can do this? In many ways I’m excited to no longer be a student, to finally feel like I have a place, and like I’m no longer a fly on the wall.
When I think back to the first day of medical school, I’m not entirely sure how we got here; how and when everything changed and came together. I think we all battle with imposter syndrome to some degree, especially in the early years. After feeling out of place for so long, it’s heart- warming to reflect on how much I’ve grown and how much I’ve learnt. I did make the right decision all those years ago.
I also appreciate that medicine is not everything. Finding happiness and meaning outside of work is important, especially as we approach a busy and emotionally demanding internship year. Take time to check-in with yourself and prioritise self-care; watch that movie, go to that restaurant, take up that new hobby.
Most of all, I hope you’ve learnt that you’re worth it, that you belong. You will make an incredible doctor. As long as you show up, try your best, and show genuine care for the people around you, the world truly awaits.

These comics have been shared with The Auricle by our anonymous creator Regina Phalange. This piece featured in The Auricle‘s October-December Edition in 2022.


This photograph, captured by Christopher Photopoulos, received an Honourable Mention in the Visual Art division of the 2022 MIPS x Auricle Creative Writing and Visual Art Competition. Christopher says, “when we seemingly drown in our everyday life as we navigate this ocean of possibilities, sometimes all it takes is a walk on the beach to come up for air — to breathe is to reflect, to stay grounded, to change.” This piece featured in The Auricle‘s October-December Edition in 2022.
Tides of Change
[Aerial drone footage. VIC, Australia. 22.06.22]

This piece by Fathima Ijaza Irzan featured in the Visual Art division of the 2022 Auricle x MIPS Creative Writing and Visual Art Competition, receiving an Honourable Mention. This piece featured in The Auricle‘s October-December Edition in 2022.


This piece by Laura Smith received an Honourable Mention in the Creative Writing division of the 2022 MIPS x Auricle Creative Writing and Visual Art Competition. Laura describes it as a “piece on uncharted waters as a medical student equipped only with the skills of two pre-clinical years.” This piece featured in The Auricle‘s October-December Edition in 2022.
“Presented with bilateral pulmonary embolisms. CT scans came in this morning and showed stage 4 lung cancer. She’s probably got about 6 months to live. If she’s lucky.”
“A walking ad for Quitline.”
Laughter from the team of respiratory clinicians.
“They should take her picture for the back of the box while she’s still alive.”
Medical students shadowed the doctors, lingering behind and doing their best not to get in the way. Struggling to find the situation humorous but not wanting to be impolite, Eloise halfheartedly attempted a smile.
Two years of textbooks and artificial clinical scenarios with paid actors hadn’t prepared them at all. Eloise thought of anatomy lessons, of the hours spent dissecting pungent corpses and appraising ‘specimens’- human body parts chopped up and laid out on tables.
Confronting was barely the right word to use after everything they’d seen in their first week in the hospital.
When the ward rounds were over, one of the younger doctors approached the students and suggested they visit the patient in bed 32.
“Take a medical history. Just ask her why she’s in here and make sure to have a listen to her lungs. Let me know what you find.”
Pacing the hallway just outside bed 32, Eloise wondered whether it was facetious to pry, poke and prod at a woman who had limited time left on earth and was faced with the task of accepting her own mortality. Her ward buddy grew anxious with her, twisting his stethoscope and inspecting it closely, as if to find moral guidance within its diaphragm.
“Can I help either of you?”
Brash and unforgiving, the ward nurse peered down upon the two 3rd-year medical students, her overbearing presence immediately quashing their ethical doubts.
“We’ve been sent by the Resp team to have a chat with Mrs Greenwood, are we alright to head in?”
Clearly unimpressed by their hesitance, the nurse let out an exasperated noise and nodded her head in the direction of bed 32.
Flowers drooped in the corner of the room, their presence gaudy and somehow melancholic against the harsh white hospital walls. A tiny television screen hanging from the roof was tuned into a reality show that Eloise’s mother would have described as ‘American trash’. Mrs Greenwood’s attention barely shifted from the show as the students introduced themselves and obtained her consent for a medical interview and examination.
Her bedside table was littered with empty food containers and medications, and a pile of books and magazines. Eloise’s attention was drawn to one particular title- ‘Turning a new leaf; how to embrace a healthy lifestyle!’.
“If you don’t mind Mrs Greenwood, could we turn off your TV for a moment to ask you some questions?”
“It’s June, dear.” The patient gave Eloise a warm smile as she switched off the screen and indicated for the students to continue in their history taking.
“First of all, could you tell us why you’re in hospital at the moment?”
“Well I’m still asking myself that. I was fit as a fiddle a week ago when I started noticing a sharp pain in my chest.”
“And your husband called an ambulance, is that right?”
“Yes, my Dad died of a heart attack, so of course that was the first thing I thought of. Lucky it wasn’t that! I had a couple of scans and apparently I’ve got clots in both my lungs.”
“And did they notice anything else on the scans?”
June didn’t notice the tremble in Eloise’s voice and the way her eyebrows rose and furrowed in strained sympathy.
“Nope. I’m all good. I’m on tablets to thin out my blood and I’ll be back home tomorrow. My husband’s coming in later today and we’re having a meeting with the doctors to plan my discharge.”
Eloise’s teeth clamped down on her tongue, a metallic taste filling her mouth and drowning the tears she felt rising in the back of her throat. Her fate would be revealed later today, in what hospital staf referred to as a family meeting. Mr Greenwood would have already received a ‘warning shot’; a purposefully ominous phone call instructing him to come in to the hospital immediately to discuss his wife’s health. Maybe there’d be others too; siblings, children, even grandchildren. They would all suspect something was wrong. But June still had no idea.
June said the whole experience in hospital had caused her to have a ‘health enlightenment’. Though distressed initially, she had managed to conjure optimism by committing to lifestyle changes she thought were probably long overdue.
“I’ll be quitting smoking, obviously. Don’t want anything else nasty turning up in my lungs. But I’m also taking the opportunity to start exercising more and eat lots of fruit and veggies.”
Blurry photographs crudely cut out and blue-tacked to the wall were almost unbearable to look at when Eloise entered the room, but now she refused to avert her gaze. Anything to drown out the fleeting hope of a woman on her deathbed. She wasn’t here to read the chapters of a book she already knew the ending to.
In medical school, they’d been warned against medical paternalism; doctors being accused of playing God, of defying patient wishes, of intervening in the natural course of life. Right now, Eloise felt close to divine power as she forced back the words that would bring an end to June’s world. Neither of the students could bring themselves to touch her so they thanked her and took off without listening to her lungs.
An elderly man, perhaps in his late 60s, wandered down the corridor with a bunch of mismatched flowers, roots still attached from where they were yanked out of the garden. Eloise thought she saw a glimmer at the base of his eyes as he turned and entered the room they’d just left.

This gentle, subtle poem by Zoe Weimar, titled “Quieter Now” transports us to a moment of tranquility on a hospital ward. It received an Honourable Mention in Creative Writing Division of the 2022 MIPS x The Auricle Creative Writing and Visual Art Competition. Zoe describes it as “a poem/sonnet inspired by experiences placed on birth suite, and moments of beauty that occur there.” This piece featured in The Auricle‘s October-December Edition in 2022.
It is much quieter now than before
The room had filled, filled, filled
And then drained. Closer night draws.
Though rustling blankets murmur amongst themselves, the air is still
Swaddled warm and wearing a striped hat
Something tiny and new sleeps
In her arms, as we marvel at
His newness, her strength. The teabag steeps
Of course, there’s beauty in first breath, first touch
Yet those less-remembered moments in-between; with kind words said
And hands held tight and laughter shared, hold such
Intangible softness. She shifts further up in bed
The sound of my steps punctuates the room’s quiet, as I bring her the hot mug of tea
To brew it is my privilege, however small or unskilled an act it might be

“The Caretaker” by William Upjohn received an Honourable Mention in the Creative Writing division of the 2022 MIPS x The Auricle Creative Writing and Visual Art Competition. William says, ‘I wrote a short science fiction/horror story, set on a deep-space satellite in the distant future. It is titled “The Caretaker”.’ This piece featured in The Auricle‘s October-December Edition in 2022.
Caretaker’s Log:
02/08/54,675 C.E (Estimated Earth Date)
This is likely to be my final statement. I have not made many other entries to this log, a decision that I now regret. I am not sure who, if anyone, will read this. I seek only to explain what happened on my satellite, and to enlighten those who would otherwise not understand what lead me to undertake what I did. I do not seek forgiveness, because I know I have not done anything wrong. This is not a confession.
I am not sure how long until my satellite will be found, or by whom. In case this part of our history is forgotten by those who discover it, I shall provide a brief amount of context. In the year 54,345 C.E, our sun began expanding at a rate far, far greater rate than our scientists had anticipated. This gave us around 50 years to escape our planet and retreat to a safer distance, before life on earth became unviable. The decision was made to place as much of the population as possible into a hibernation-like stasis or “cryo-sleep”, and put them safely on millions of satellites in orbit, far away from the now malignant sun. Most, including mine, were placed in orbit at a distance similar to that of the former planet Pluto. The plan was for other, exploratory spacecraft to search deep space for a new planet with conditions favourable for colonisation. Once this new planet was found, the cryo-sleep satellites would be brought over and reawakened.
Using almost light-speed travel, the estimated time for this mission was between 60 and 80 Earth years. This timeframe has come and went, without transmission or signal from any of the thousands of exploratory craft. It seems overwhelmingly likely that all missions have ended in failure.
My satellite is one of the smaller models placed into orbit. It initially housed 100 individuals in cryo-sleep. It is almost entirely run algorithmically by AI; however, the decision was made to include a single human overseer to ensure the smooth running of all the ship’s functions. This overseer, or “caretaker” as we came to be colloquially known before launch, could override any direction from the ship’s AI, to prevent computer glitches or malfunctions from jeopardising the survival of the satellites’ occupants.
Being a healthy young male with a favourable genetic profile, I was chosen to be the caretaker of my vessel, a position I was honoured to accept. While the position was demanding, and the prospect of decades of isolation not very attractive, I was assured that personalised neurotropic medications would be administered to ensure my mental wellness was preserved. The fact that I was unlikely to secure a position on a satellite otherwise, and be left on the soon-to-be uninhabitable Earth also contributed greatly to my decision to accept.
The first few decades of orbit were largely unremarkable. I developed a routine of monitoring the sleeping passengers and certifying all vitals were in the desired range soon after waking. I then spent my time confirming our orbital path was optimal, supervising any maintenance activities, and generally ensuring that the satellites processes ran smoothly. In order to preserve power, communication with other satellites was completely ceased after the first year. As a result, I had no contact with other humans, only being able to communicate with the satellites’ AI. While this might have been emotionally detrimental to a normal person, the medications I took daily ensured that my mental state remained favourable.
Though the 24 hour cycle of days was now arbitrary, I kept to a pattern of 8 hours sleep followed by 16 hours of waking, trying to avoid the cognitive disturbances found in disrupting the normal circadian rhythm. I ate three times per day, and bathed regularly. The temperature of the satellite’s internal spaces, where I lived and worked day-to-day, was kept to around 14 degrees Celsius. This low temperature was maintained in order to slow metabolic activity and decrease the rate of aging. This meant I was permanently slightly cold – though this is a small price to pay for the supposed increase in longevity.
It wasn’t until my 35th year in orbit that the first complication occurred. During my annual health scan by the satellite’s medical AI, a sizeable adenocarcinoma was found in the hilum of my right lung. This most likely due to exposure to radon, an inert gas that can leak from small nuclear reactors such as the one powering my satellite. While I was not yet experiencing symptoms, it was still a threat to my wellbeing, and I elected to have it surgically removed. The satellite had multiple automated surgical robots, capable of performing almost any surgical procedure at a standard far exceeding human surgeons. Multiple passengers in cryo-sleep had already had procedures performed on them by the machines. They were not even awakened from their stasis – part of the contract for being placed into cryo-sleep involved consent to any procedure the ship’s medical AI deemed necessary.
The operation was a success, at least initially. The tumour was resected completely – however, 4 years later, I developed more tumours, this time spread throughout both lungs. Breathing was becoming increasingly difficult, and I experienced haemoptysis on a daily basis. This presented a clear and present threat to my life, and subsequently to the functioning of my satellite, and to the lives of all those under my care. The only possible treatment was a lung transplant.
While my subsequent actions may appear unethical, it must be kept in mind that my death would certainly jeopardise the lives of all those on my satellite. I could not allow this to happen. It was a difficult decision to make, but ultimately, it is a decision that I stand behind. I took no pleasure in making this choice, and to this day I find the whole process distasteful. I detail my decision here not out of pride, but simply to allow future readers to understand what happened.
I elected to take the lungs of one of the passengers. It was a very grim choice to make, but I eventually settled on those of a 55-year-old man, whose name I will not mention out of respect for the dead. He was a healthy adult male who didn’t smoke, and the medical AI suggested that his organs made the most favourable match. This wasn’t truly necessary – the immunosuppressive medications I would take made virtually any donation viable, although matching did reduce the risk of complications. I cannot detail all the factors that went into my decision, but after 2 weeks of deliberation, accompanied by increasingly severe symptoms, I finally made the decision to go ahead with the procedure. I had to manually override the medical AI, but the surgery went off without issue. The donor was not brought out of cryostasis during the procedure. He did not suffer.
The new lungs were completely successful, and it was almost a full decade before I needed another organ donation. Perhaps due to my constant use of neurotrophic medications, my renal function had deteriorated to a dangerously low level. I required a transplant. Selecting a donor was far less ethically difficult this time, as transplanting a kidney would not result in the donor’s death. For the sake of brevity, I will not give the details of this donation, nor for any of the subsequent ones. Again the procedure went by without issue. The donor was in cryo-sleep for the entire surgery, and was successfully returned to her cryo-pod afterwards, without ever knowing such a procedure took place.
I will not give unnecessary detail about all the subsequent transplants. Initially, at least, I held out as long as possible without using any more organs. However, as the length of my mission extended longer and longer past the expected end point, the aging process resulted in the inevitable deterioration of my body. The successful running of the ship was paramount, and this success was dependent on my input. As such, any and all actions I undertook were necessary, and in my opinion ethically sound. While it appears increasingly likely that I will not have to explain my actions to any individual in my lifetime, I would like to emphasize that I stand by the decisions I made.
Over the almost 280 years that I have now been caretaker of this ship, I have had to extend my lifespan much, much further than would be natural. I have considered bringing a passenger out of cryo-sleep and training them to be a new caretaker, allowing me to finally give up my position, but this is not a viable alternative for many reasons. The most important one, in my opinion, is that the neurotropic medications, which allow me to function under enormous psychological strain, are personalised to my neurological profile. They would not be effective in any other individual. It seems overwhelmingly likely that another person in my situation, faced with the cold, claustrophobic, completely isolated conditions that I live in, would be made insane. I think of myself as something like a deep sea fish, one that inhabits unimaginable pressures without issue. Any normal organism, however, would be crushed.
In order to prolong my life, I have received new transplants of almost every viable organ in my body, as well as various tissues and vessels. I have been through 48 sets of lungs, 40 hearts, and 44 pancreases, as well as countless skin, marrow and vessel grafts, just to name a few. I am not wasteful – I do my best to maximise the number of organs I can use from every donor, and try my best to prolong the use of every organ that I receive. It is difficult, however; as my age increases, the amount of use I get from each transplant lessens. While my first new heart lasted me over 30 years, currently, a new heart will only last me four. This has meant that I am requiring new donations more and more frequently, a situation that is as regrettable as it is inevitable. It brings me great emotional pain to accept organs from those I am supposed to take care of, and were it not for my medications I likely would not be able to cope. These actions must be undertaken to fulfil my duty as caretaker.
I have all but given up hope of rescue – I have not received any transmission, from another satellite or any other craft, since the silence descended all those years ago. I have considered the possibility that my equipment is faulty, and all the other ships have been rescued while I remain here alone, unable to receive the signal. These idle speculations serve no purpose but to heighten my distress, so I avoid them as much as I can.
I imagine that my story is not unique, and that every other living caretaker has had to make the difficult decision that I have. My supplies are dwindling: I have only 20 more untouched donors to use, and my needs are increasing with every year. I do not know what I will do when I have run out, when my satellite has no more passengers and I am left truly alone, orbiting a dying star. According to my ship’s navigational system, we have almost finished our first complete orbit around the sun. I only wish my satellite had windows, that would let me look outside and see the stars. It has been far, far too long.
That concludes all that I wish to say. This is not a confession.
<end of transcript>

In the July-September Edition instalment of Humans of Medicine, we spoke to Ruby Doherty and Jess McKie. The brains behind the 2022 MedRevue, these two possess a creative and humourous side that shone through in two extremely successful and well-received shows in August. We hope you enjoy their insights into the process of creating such a stunning performance.

First of all, congratulations on two magnificent shows! The reaction from audiences was hugely positive. You must be relieved that everything went so well?
Yes, we are very relieved! Especially after having 2 years without a show, we did feel some pressure to really come back with a bang. The audiences were fantastic, we’ve been so lucky to have had so much positive feedback about the show and we are really grateful to everyone who supported us throughout the year and came to the show. Everyone has been so kind and supportive! We want to give a big shoutout to the members of faculty that came and have reached out since, we really appreciate that they take it all in such good humour and continue to stand behind MedRevue. Their support means a lot! The entire team at every point in the process did such an amazing job and the whole committee is just so proud of the show we were able to put on.
The theme for this year’s MedRevue was “The InMEDibles”. What was the inspiration for this theme?
Every year at the MedRevue AGM (which everyone should come to this year if they are keen to get involved), we have a brainstorming session for the theme for the following year’s show. We discuss many different theme options and consider possible plot lines and then everyone at the AGM gets to cast their vote. The Incredibles was a particularly appealing theme as it was a story that lent itself to a more ensemble cast, which means that we are able to create a wider range of opportunities for more people to be involved.
Can you take us through the process of designing a show?
The very first step is our AGM. This happens at the end of every year after the show. Our AGMs have an open-door policy and everyone is welcome. At this meeting, we recap the show from that year, do all the boring committee things, elect the new committee and select a theme for the following year’s production. The incumbent committee then gets to work over the summer and early the following year planning the script, looking for a venue for a show, sorting out costumes, budget and all the behind-the-scenes stuff.
Next, the creative holds auditions and then once we have our cast, dancers and band we set to work with rehearsals throughout the year where our creative, vocal, and musical directors as well as choreographers coordinate cast, dancers and band to bring the show to life. Meanwhile, our technical team and production team organise the theatre, ticketing, costumes, sets, marketing, promo, lighting/sound design, etc. After about a week of tech/dress rehearsals in August/September time, we then have finally put on a show. It really is a huge team effort and is so much fun to be a part of.
The InMEDibles was really, really funny. What’s the secret to writing such an entertaining script?
The secret of a good script is having a strong cohesive scripting team right from the brainstorming period. Then once it’s on paper it is important to allow time in rehearsals for the cast and creative director to work together to ensure that the jokes and storyline work on stage. A big part of the comedy of MedRevue is also developed throughout this time, as the actors put their own spin on the jokes and the physical comedy is also added. This rehearsal period also allows us to get feedback from cast and crew members in all the year levels about what has happened in their year what they want to joke about and incorporating these things into the script.
Overall, we aim to make sure that the jokes are funny, understandable to a large audience, but also that the jokes are never personal or mean spirited. We focus on incorporating issues relevant to each year level, incorporating jokes that are both med and non-med related so that friends and family can also laugh even if they’re not medically inclined and we love a gentle jab at faculty every now and then.

There are so many moving parts to putting together a show like MedRevue. The script, singers, dancers, band, promotion, venue hire and all the rest! How on earth did you coordinate it all?
This would not be possible without our amazingly dedicated committee who worked very hard to put this show together. It was also helped greatly by a very strong partnership, trust and great communication between us as creative director and producer. Having worked together as co-creative directors last year, we had already had a chance to develop a strong working relationship which we were able to build on further this year. As creative director, Ruby was responsible for coordinating the cast, band, dancers throughout the rehearsal process, collaborating with other creative committee members and all that was necessary to bring the show to the stage. Jess as our producer was responsible for coordinating the committee and making sure everything was happening behind-the-scenes in order to ensure a production could on stage with an audience. Overall, the most important thing was teamwork between all members of the production and especially our incredible committee.
Both of you were responsible for creating last year’s MedRevue as well, which unfortunately couldn’t go ahead. What was it like to put so much effort into a show that didn’t come to pass?
It was very disappointing as we were so close to our performances, with less than 2 weeks from showtime. Tickets had been sold, the show was finished and everyone had put in an incredible amount of effort. It was a great show that we were all really proud of. It was disappointing that it couldn’t go ahead and that we couldn’t reschedule for later in the year but it just became impossible due to the lockdowns, graduations, exams, etc.
However, we had discussions with the cast and crew it was felt that we had all had the experience of doing MedRevue. Although audiences didn’t get to see it and this was disappointing, we all still had the experience of getting to know and work with one another and really engage in that creative outlet. As much as MedRevue is a performance, it is also so much more than just a 2 night event, it’s a 12 month long process between a large team of people you become close with and have a lot of fun with along with the way.

Why should people get involved in MedRevue?
There really is something for everyone! Whether you’re someone who prefers to be on stage, offstage, play an instrument, or work behind the scenes in tech or backstage, there’s something in MedRevue for you. You don’t have to sing, dance or act or have any experience, it’s all about enthusiasm, having fun, making friends and doing something a bit creative. All we ask is that you bring yourself and your sense of humour. It’s also a really great way to meet and become friends with people in other year levels and you can learn a lot from those people. You really get to know the people you do MedRevue with and we are not sure there is another subcommittee that fosters connection and relationships in the same way MedRevue does, purely due to the amount of time spent working together towards a very fun common goal.
MedRevue is a welcoming space for everyone. Our community is very diverse and you don’t have to be massively into musical theatre to be involved, we have a very wide range of people who come to MedRevue and are involved in MedRevue and all are welcome. As it’s not academic focussed, it is a more light-hearted subcommittee experience, people have a lots of fun and look back on their MedRevue experience very fondly.
If you are keen to know more or want to get involved please like, comment, and subscribe and stay tuned for notice about the 2023 show. Follow Monash MedRevue on social media, all updates with be announced on Facebook primarily.

Shefani Perera is a member of the Academic Team of the Psychiatry Society of Monash (PsySOM) Committee. In this piece, she analyses the current mental health system in Victoria and some of the key challenges it faces. We hope you find this piece, which first was published in The Auricle’s July-September Edition, an informative read.



This poem was written by Virginia Su, Co-Chair of MUMUS Community and Wellbeing, and was initially published in The Auricle’s July-September Edition.

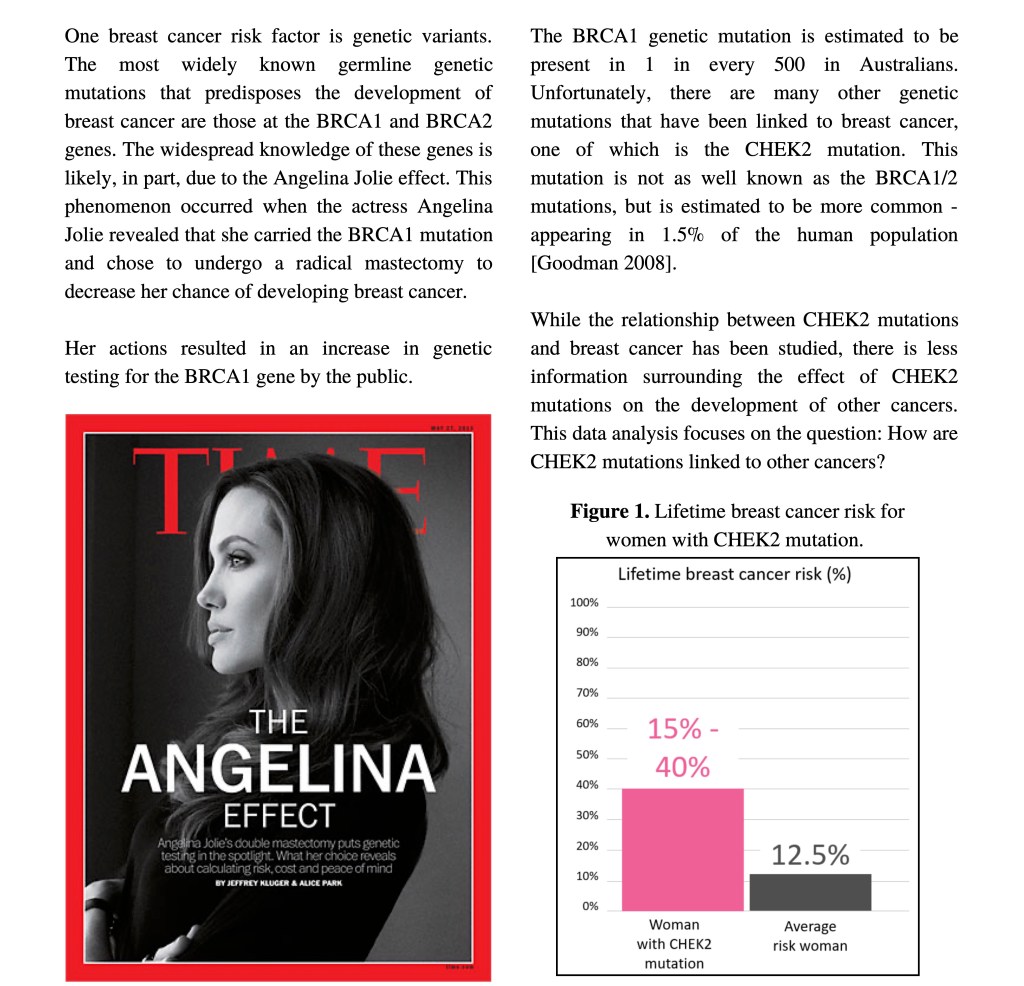
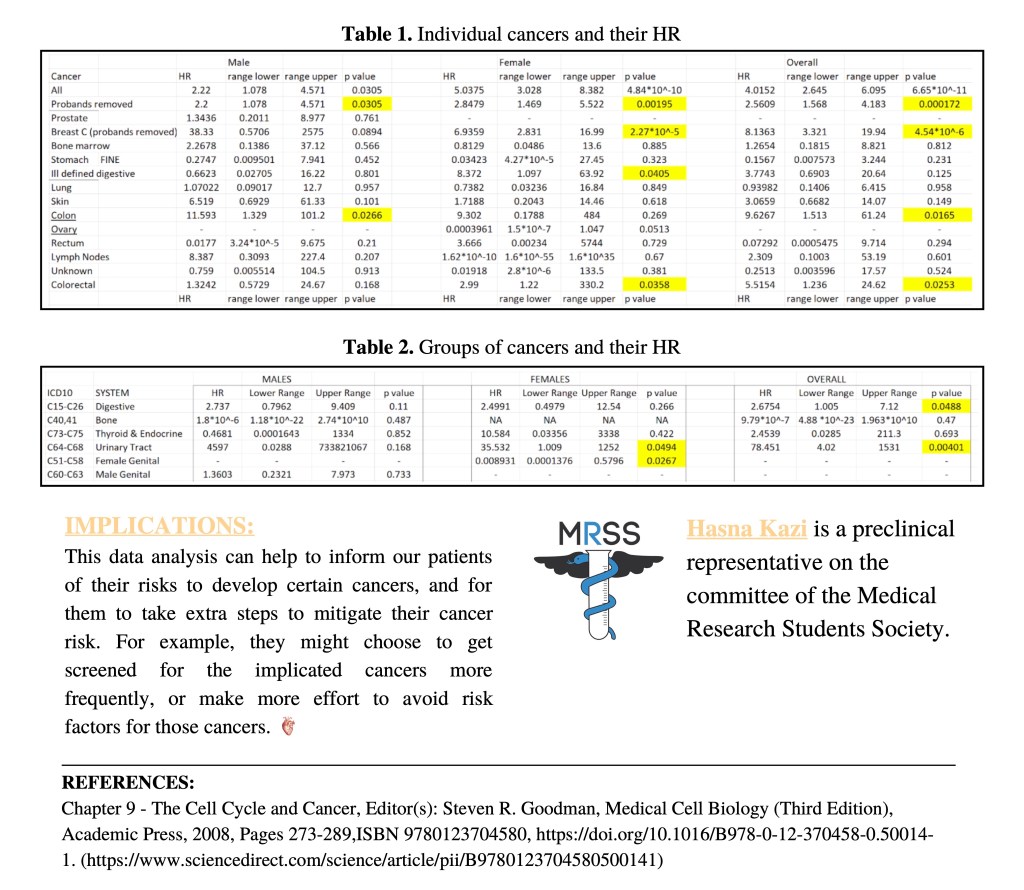
In this piece, Hasna Kazi, a preclinical representative for the Medical Research Students Society, shares with The Auricle some original research analysing the link between the CHEK2 gene and cancers. This piece originally featured in our July-September Edition.
Author’s note: Acknowledgement of supervisor – Dr Shuai Li at the Breast Cancer Unit, Centre for Epidemiology and Biostatistics, University of Melbourne. Dr Li was a brilliant and understanding supervisor and I cannot thank him enough for this opportunity.


This fascinating piece, titled “Empty Celebration” and submitted by Lois Segund-Beloved, received third place in the 2022 MIPS x The Auricle Creative Writing and Visual Art Competition.
All winners can be seen in The Auricle’s July-September Edition.


“Retro Funk” by Charlotte Raberger received second prize in the Visual Art division of the 2022 MIPS x The Auricle Creative Writing and Visual Art Competition.
Artist’s note: Encompassing metamorphosis, these sculptures repurpose old kitchen utensils to create something new and ‘funky’. The black and white painted pattern connects the figures, symbolising commonalities between humans despite so many differences, represented by the variety of body shapes and vibrant patterns.
All winners can be seen in The Auricle’s July-September Edition.


A deserving winner, the piece featured below received first prize in the Visual Art division of the 2022 MIPS x The Auricle Creative Writing and Visual Art Competition. It is titled “Reflection”, created by Anna Noe.
Artist’s note: Reflection describes the simplest concepts of identity, the name you are given at birth, cultural heritage and own persona. The symbolism relative to my artistic ideas, the jasmine flowers, Arabic letters and culturally significant black stones are placed behind the portrait allowing them to ambiguously carry the essence of an identity rather than an outer persona, showcasing a glimpse beyond the veil.
All winners can be seen in The Auricle’s July-September Edition.


The third placed entry in the 2022 MIPS x The Auricle Creative Writing and Visual Art Competition is a powerful poem by Tessa Quinlan, titled “Never Let Them Fall”. We’ll let you unravel the subtext that emerges through the clever writing and structure.
If you would like to see all winners in the competition, see The Auricle’s July-September Edition.

The 2022 MIPS x The Auricle Creative Writing and Visual Art Competition featured some amazing work – here we are excited to share with you the piece that placed second in the Creative Writing division. Titled “I am Everyone” and written by Khue Le, it is a truly moving piece. If you would like to see all winners in the competition, see The Auricle’s July-September Edition.
Good morning! My name is. I’m a medical student.
I’m the daughter of parents who called me downstairs to greet guests I didn’t know and reminded me to speak louder when I said my hellos, so to you, my care and respect comes freshly baked as a “good morning”. I am the girl whom my mum shows her love to through a plate of sliced apples and washed grapes when I’m studying, through a thermos of tea left out for a few minutes so it’s the right temperature to not burn my tongue and through the almost sickeningly sweet condensed milk with toast she makes when I’m sick. So I am careful to pull the curtains close when it’s time to examine you. I tuck in the covers after pressing your shins for pitting oedema. As I talk, I am righting the chair, pushing the glass of water closer to the table centre, moving your bag into an accessible spot. I don’t want you to trip.
I’m an immigrant kid who in Prep, drew lines and hats and moustaches on their letters in class because the alphabet was supposed to have accents. On Footy Day at school, I’m the kid who repeated the mysterious word, “Collingwood”, to anyone who asked what football team I barracked for and had a boy ask me why, if so, I was wearing purple, orange and pink stripes. There are more football teams, I said in embarrassment. So I take extra care to speak slowly and gesture wildly, opening and closing my palms to indicate a beating heart, when I know English is not your first language. In my head, I am running experiments on ways to best explain congestive heart failure to you.
I’m a university student who spent two fifths of their course at home, nostalgic for dreams of studying at libraries and practising auscultation on real people. I’m the blundering person on the team who stumbles on anatomy questions because the anatomy I studied had been colour coded with red arteries and blue veins. Being in a pandemic means loneliness has visited me. It also means I listen hard and carefully when you tell me your story and I try to know you as you were before you came here. The grandfather who spent more than half his life on a boat, the neighbour who walked her little dog to collect the mail, the engineer who built some of the protocols for the equipment I now see in hospitals.
Having a medical condition can be lonely. I didn’t want you to feel trapped in your existence as a patient.
And if you are resigned to the long waiting list and the medication expenses, if you endure pain by sheer will and hasten to get out of hospital so you can start working again to provide for your two daughters, I am reminded of my dad. My dad and his calloused hands. My dad whose working hours were dictated by the ending of the Sun’s rays. I am the older sister who had memorised chip packets in order of their monetary value so I could buy the cheapest one. I’m the 10 year old who grew up defining her financial status by the snacks she couldn’t afford. So I recognise, somewhat, your hesitancy to travel when petrol prices are high, your helplessness when the doctor says you need to attend more check-ups, the determination to overcome this by your resolute jaw and the quiet concentration as you face the window.
When I get home, I will think back to this moment and be angered by the ways spaces have been designed to keep you and countless others out. How, sometimes, it must feel like health is for everyone, except these spaces have told you that you are not everyone.
I am all the experiences leading up to this interaction. I am everyone I have encountered and so, I am the medical student who went into medicine with hopes of redesigning these spaces. Hoping that the next you I meet and all the yous after will access health more easily both in and out of hospital.

We are delighted to share with you the first place entry for the 2022 MIPS x The Auricle Creative Writing and Visual Art Competition. The winner was Natalie Evans, with a piece titled “Stardust” in the Creative Writing Division. We hope you enjoy this fascinating read as much as we did. If you would like to see all winners in the competition, see The Auricle’s July-September Edition.
Meditations on Medical Dissection
It is 8am on a Thursday morning and in front of me lies a bag on a metal table. I am nineteen years old and never even been to a funeral. The room has very good ventilation – but an unsettling odour still lingers and there are small puddles on the floor. I am standing there with three other medical students – my anatomy group. About ten more groups in the room stand before their own dark blue bags. We are told to feel the bag, to orientate ourselves with the stiffness beneath. We do so, patting at the bag gingerly with our gloved hands. Then it comes time to unzip.
§
Long ago, another’s hands hover tentatively over a similar body – except this body is that of an executed criminal, his soul left back at the gallows where his breath disappeared into silence. The person crouching over the already decaying corpse is considered a criminal for this act of bodily desecration. This is in Ancient Greece in the second century BC, where medical dissection is recognised to have begun.(1) Those who wished to access bodies for dissection were forced to obtain them via illegal means such as grave robbing and body snatching.(2) A change in attitude towards dissection began in the third century BC, when royal patronage allowed dissection in Alexandria, Greece, in order to establish it as a ‘glittering centre of literary and scientific learning’.(1) Prior to this, official exploration of the human body was superficial both literally and metaphorically.
However, this small sliver of discovery was brief, and what followed was a retreat into the old ideas and beliefs surrounding dissection. Religious taboos and societal notions restricted scientific progress until there was a ‘revival’ in Medieval Italy at the outset of the fourteenth century.(1) At this time, religious authorities gave permission for human dissection conducted within university premises, and this occurred once or twice a year using executed prisoners.(3) In the fifteenth century, many physicians obtained bodies for dissection by unethically convincing families that their loved one required a post-mortem, which in most cases was untrue.(4)
It is not only medicine that has profited from the innards of man being explored. The artistic sphere was also responsible for pilfering the dead to further the ‘portrayal of [the] human figure’.(1) Leonardo Da Vinci, Michelangelo, and Baccio Bandinelli were all practiced in stripping back the flesh of man’s clockwork and uncovering what makes us tick. With such a dire demand yet limited supply of cadavers, even those still living felt under threat of being murdered for their bodies. Although individuals living in poverty were the main targets, there is a rumour that a Spanish aristocrat was set upon and dissected whilst his heart was still beating.(1)
Thus, human dissection has evolved from being a criminal act bestowed upon criminals, to a consequence of poverty, to a process of informed consent and respect.
§
Prior to entering medicine, death had been imagined as a stillness, an ending with closed lids, distant weeping, church bells, a tableau of black. In the movies, death transpired as a mise-en-scène of violence with gunshot or stab wounds, necks bent at bizarre angles, and scarlet pools spreading over wet asphalt. There had never been a time when the idea of death conjured up forceps, surgical scissors, sinks, gloves and slippery floors. But there we were, tentatively hovered around a cadaver, hands within white or blue gloves, and a tray of surgical instruments gripped nervously. Now we’re unzipping the bag and so is everybody else. I start seeing glimpses of the bodies and I wonder if anyone will faint and if so, that person better not be me.
Our donor was a man. His face was covered. Nausea needled my stomach because this was not how cadavers were supposed to look. Didn’t cadavers look like the preserved sections in glass we had studied in specimen class? Why did these bodies appear as if they had simply fallen asleep? However, after the initial shock, we became wholly invested in writing our dissection plan on the whiteboard and beginning the hunt for the elusive brachial plexus. After one hour we were all at the sinks, turning the taps to let loose streams of water which cascaded down the long metal basins. The sinks reminded me of the troughs that fed farm animals, and the crush of students washing their hands made me feel like I was part of a medical student herd.

Twice a week we shrugged on lab coats, donned gloves, fit blades into scalpels, and collected the scissors and forceps on the tray. We were practiced at writing on the whiteboard the list of tasks for the day’s dissection, unzipping the body bag, receiving a handover from the previous group about what they had accomplished, and beginning.
We also became adept at the unspoken things, like learning to hold your breath whilst opening the body bag, eating lunch even if you are not hungry beforehand, and remembering to wear shoes that you do not mind touching the fluid on the floor. At some time, at some moment – standing amongst both the living and the dead had changed from ordeal to routine.
One member of my anatomy group named our donor Sir Gregory. This christening into the afterlife was adopted by many other groups and for us, the name stuck from then on. We were very lucky to have Sir Gregory as he possessed clear anatomy and lacked any confusing anatomical variations. One day, an echo of his life unexpectedly emerged when we stumbled upon a tattoo on his arm of a name. We could only guess at what this name might have meant to Sir Gregory, a secret locked within his earthly vault.
Survival is the human body’s most gifted architect. Every hollow, chamber, space, layer of muscle, skin or outline of bone has been expertly crafted to imbue the greatest working efficiency and survival edge. Gazing down at this accomplishment of biological machinery, I could only imagine the sight if blood coursed within the vessels and the body performed its triumph of animation. However, with this complex feat of engineering comes a very weighty caveat – with such intricacy comes great capacity for error. This sentiment is true for many themes of life – but is equally and most pertinently true in the physiological nature of life itself. In this way, the benefits of dissection became very clear to me very quickly. The secrets of the human body were right before our eyes – presented in a form which a textbook could never hope to reproduce. Most startling was the discovery that the human body does not possess colour coding and that as each person differs mentally and physically, anatomically the variation can be endless.
Over time, my anatomy group began to develop the ability to differentiate between arteries, nerves and veins based on appearance and feel. To hold an organ, feel the elastic bounce of an artery, fashion a window in the atrium of the heart then view the valves within – these experiences are the capstone of dissection. It was in dissection where I realised that “heartstrings’’ are a real structure. Anatomically, your chordae tendinae, colloquially known as heart strings, are connective tissue cords that connect small papillary muscles to the valves in the heart. These small strings anchor your valves whilst the heart pumps blood. Thus, if something “pulls at your heartstrings,’’ I imagine some force pulling back on these strings like reins on a horse, causing the heart to buck under the strain of such emotion.
There is also an importance to dissection that is separate to the anatomy. To physically cut another human being does not come naturally – so as a student you learn how to cut with compassion. A new level of empathy develops to ensure you are both respectful to the donor and to minimise damaging a structure that might be required later. Simultaneously, the student must be confident when attempting the dissection, as if they are too anxious about each tiny incision, nothing gets done and precious time is wasted. Although it seems unkind to alter a person by such physical means, the purpose of the whole exercise is to learn as much as possible and ensure the donor’s contribution enhances your understanding. Some of the most important concepts our group learned were from making mistakes – mistakes like confusing the paths of major arteries – which are better to be made on someone who no longer requires their arteries than in clinical practice.
Our tutor described a case where a woman had an operation and was severely ill during her recovery. Once this was investigated it was discovered that both her ureters had been cut during the procedure, thus her body had been unable to excrete urine. It is hard enough identifying objects in a still body, let alone one that is aflush with life, however errors like these must be mitigated at all costs through rigorous training and educational experiences such as dissection.
§
One day we moved to the new anatomy building. Compared to our old building it was gargantuan, with a green speckled façade that resembled a fungus. Inside was a lot of empty space punctuated by black stairs that slashed down the middle like unimpressed eyebrows.

Seeing the donors in this new space I found I was glad they inhabited brighter and sleeker quarters. It was as if they too had been given a gift – and the snowy whiteness of it all imparted a heaven-like quality. There were also screens placed around the room, on which our tutors could illustrate a structure from a specific donor to the whole class. In a sense – with the bright lights and screens – the donors were metaphorical film stars in a limbo universe.
§
Suddenly it was the last day with the donors who had helped us in our medical journey for two semesters (semester two of first year and semester one of second year). When I began dissection in first year, it was with a male donor who had been claimed by another group this year. This semester I had a new anatomy group and a female donor who had helped us to understand female anatomy. Our tutor told us to focus our dissection on the pelvic area – but we were also free to explore any other area so far dissected, as it would be our last chance to do so.
A timer ticked down to zero. At zero everyone returned to their donor and our anatomy lecturer conducted a minute’s silence. As silence descended we all shared a moment with the donors – silently thanking them for their generosity and the privilege they had honoured us with. I found myself imagining my donor’s life – projecting a film in my mind of someone running in the sunshine – a kindly voice – a smile.
The minute was up. Our anatomy lecturer walked down the rows announcing cause of death.
Table One – Male – 72 – Cause of Death – Multiple Organ Failure
As she read through the list I kept in mind Sir Gregory from last semester and wondered again which table he was this year. The lecturer arrived at our table. Cause of death:
Metastatic Lung Cancer
Cancer was the prominent grim reaper in the room. It is the great erratum of biology, our own cells turning rogue and militant against the life that bore them, a phenomenon that to this day we have not escaped from. We were very much surprised to learn that one of the donors was over one hundred years old, which generated a small crowd around his table. After discovering the cause of death, we were given a small window of time to view each other’s donors again, now with discerning eyes.
It was time to bid our donor goodbye. We made sure to replace her organs to their rightful place as best we could. I lowered her thoracic cage and moved the two halves of her pelvis back as close as possible to her abdomen. Then we zipped up the body bag.
§
With a new semester comes a new season, new tutorials, and new bodies. It is semester two of year two and a new workbook is provided in our first anatomy class. This time my anatomy group congregates around a different table. The man stretched before us will lend us his head and neck, and the Year Ones will simultaneously dissect the upper limb region. I realised that the other cadavers we had dissected last semester had probably been cremated by now, and this realisation made me feel as if the donors had died for a second time.
There is a 1941 film called A Woman’s Face, which stars Joan Crawford in the titular role. It revolves around Anna Holm, a facially disfigured woman who spends her life punishing the world that injured her. By chance, her path crosses with that of a doctor who specialises in restoring normal appearance to victims of facial trauma. The doctor offers to help her, pro gratis, and once she agrees the film falls away neatly into two halves – before and after the operation that changes Anna’s life. There is one line in the film that is quite magnificent. When the day comes for the bandages to come off Anna’s face – no one knows whether the operation has been successful – or whether her features will have been destroyed forever. The doctor says to Anna, ‘If this operation’s a success I’ve created a monster -’ There’s a beat as he flicks on the lamp, ‘- a beautiful face and no heart’.
The disconnect between face and soul is a concept often explored in literature, film and philosophy. We have no control over the face we are born with, and our minds and behaviours come from a deeper place – yet the face has such power to elude and seduce. However, all that beauty or distinctiveness is the equivalent of the thin crust upon a planet’s surface.
In A Woman’s Face, it unfolds that although Anna nearly crumbles into the monster she has always called herself – she ultimately chooses the path of one with a heart. Thus in the end, both face and soul are united. All of this provokes me to wonder at how our faces affect us – and how I will feel when removing someone else’s face. It is curious to note that the only part of the donor that is separately covered inside of the body bag is the face. For some reason, the face is deemed most private, and most revealing.
§
As I walk to the table of gloves I survey the room and the small but critical change in the presentation of the cadavers. The faces of the donors are visible. Standing around the table, I see that the skin of the lower right half of our donor’s face has been cut and can be retracted if need be. I had sometimes wondered, before my medical studies, what the face of somebody who had died looked like. Would their eyelids slowly shut and fall like a curtain over the eyes as life’s performance ends? The eyes are ‘the window of [the] soul,’ as described by Shakespeare who himself drew inspiration from the biblical phrase, ‘the eye is the lamp of the body.’ Would the departed individual appear calm, tranquil, or simply frozen, trapped in an expression as the winds of life changed? Now I can say that with death, the face assumes no ubiquitous, ‘deathlike’ expression. The face simply remains in a single pose that differs between donors, with eyelids that may be open or closed, and mouths that may also be open or closed.
To begin our dissection, we refer to the other side of the face, and to the depths of previous cuts – and then the belly of the scalpel contacts the skin and someone makes an incision. The incision ends up being a straight line parallel to the nose, one long cut made up of many hesitant cuts interspersed by referring to the other side and discussion like –
‘But what’s that thing there?’
‘Should we cut it?’
‘Scissors are on the tray if you need?’
‘Could it be a nerve?’
‘Am I on the right layer?’
‘Maybe a bit deeper.’
‘You did a great job.’
We all stare at the fifteen-centimetre incision that took half the class to make. Looking around, the faces on other tables were in various states of removal. In life, some people are blessed with faces of great beauty and symmetry, others possess facial features that are striking in other ways. There are faces that tell stories of intelligence, disappointment, happiness, and regret. However, in the end, at the finale of existence, everyone possesses the same ultrastructure beneath. That dimple that emerged as you smiled, the soft blush that dappled your collagenous cheeks, the wrinkling that creases the thin papery skin – they all diminish once you wade into the pond of death. They hover as in a dream, just above the rippling surface of such a pond.
§
Our final day of anatomy arrived abruptly and without warning. Everyone was taking their lab coats out of plastic bags and donning them quickly – casting everything else aside. It felt strange to wear the starchy white coat outside of the laboratory, which in normal circumstances was against the rules.
Outside in the sunlight was a photographer as well as all the anatomy tutors and lecturers.
My anatomy group linked arms as we burrowed our way through the crowd to stand on one of the tiered stairs together. As the light flashed from the camera, capturing all our cohort and the tutors together, another image entered my mind. I saw the photographs of medical students which were printed on the wall of the anatomy imaging room, the photographs my eyes had often wandered over to whilst they were meant to be observing radiological imaging. I remembered when I found the first woman in the photographs – and then a few more appeared, and more and more. I had also found myself looking at the names below the photographs and wondering where those students were now. As I stood on those steps, I wondered where our photograph would end up. I wondered if one day somebody else would stare at the grainy image of our faces and imagine who we had been.
§
Throughout my astonishing journey in dissection, I had direct experience with three donors. The first, Sir Gregory, who assisted with upper limb, lower limb and the thorax. The second, a female donor – Miss Marple, who assisted us with the thorax, abdomen and pelvis. Our final donor was another male, Obi-Wan, who bequeathed us his head and neck. When we left each day to go home, they remained. When we went to the movies or the library or to parties – they lay patiently for us to return. I used to be afraid of death, I think I probably still am – but I realise now it is the caveat that comes with life. I have seen mortality with my own eyes, and I have seen that it is the ultimate equaliser, at least in the present day. Reflecting on dissection class, eternity, and the donors who were our first patients, I have often found this quote from the 1997 film Gattaca rippling up from my mind:
‘They say every atom in our bodies was once part of a star. Maybe [they’re] not leaving. Maybe [they’re] going home’.
References:
1. Ghosh SK. Human cadaveric dissection: a historical account from ancient Greece to the modern era. Anat Cell Biol. 2015;48(3):153-69.
2. Garment A, Lederer S, Rogers N, Boult L. Let the dead teach the living: the rise of body bequeathal in 20th-century America. Acad Med. 2007;82(10):1000-5.
3. Hildebrandt S. Capital punishment and anatomy: history and ethics of an ongoing association. Clin Anat. 2008;21(1):5-14.
4. Park K. The criminal and the saintly body: autopsy and dissection in Renaissance Italy. Renaiss Q. 1994;47(1):1-33.

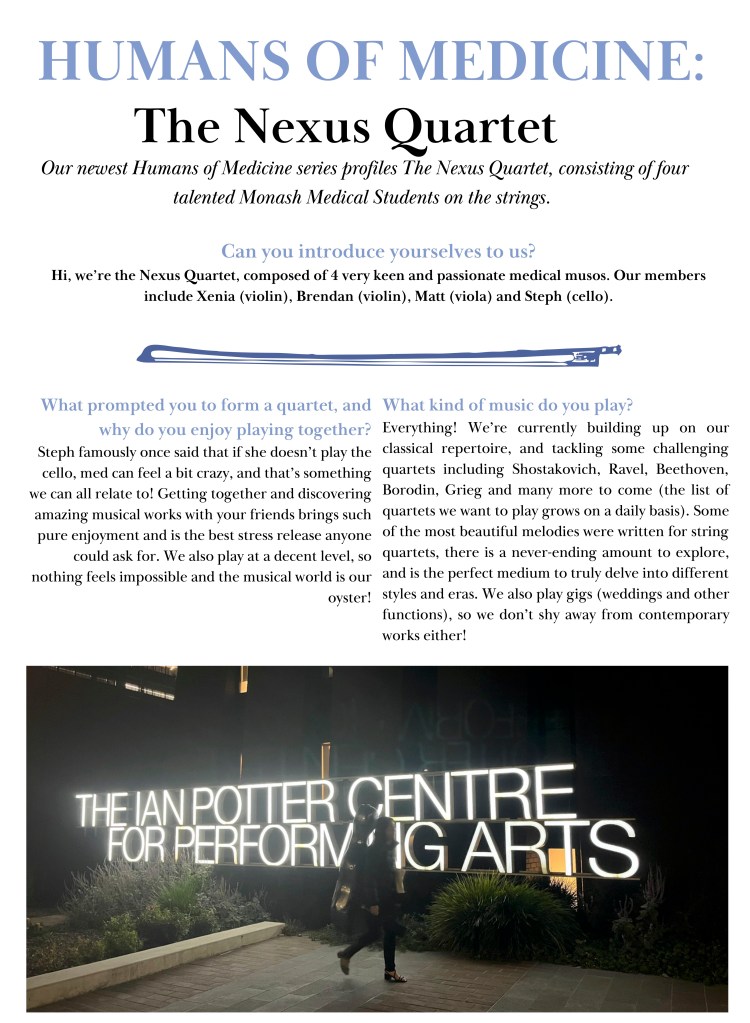
The Auricle’s May-June Edition featured this latest instalment in the Humans of Medicine series, this time profiling the Nexus Quartet! The Nexus Quartet is a group of talented musicians and Monash med students. Read about their story here!


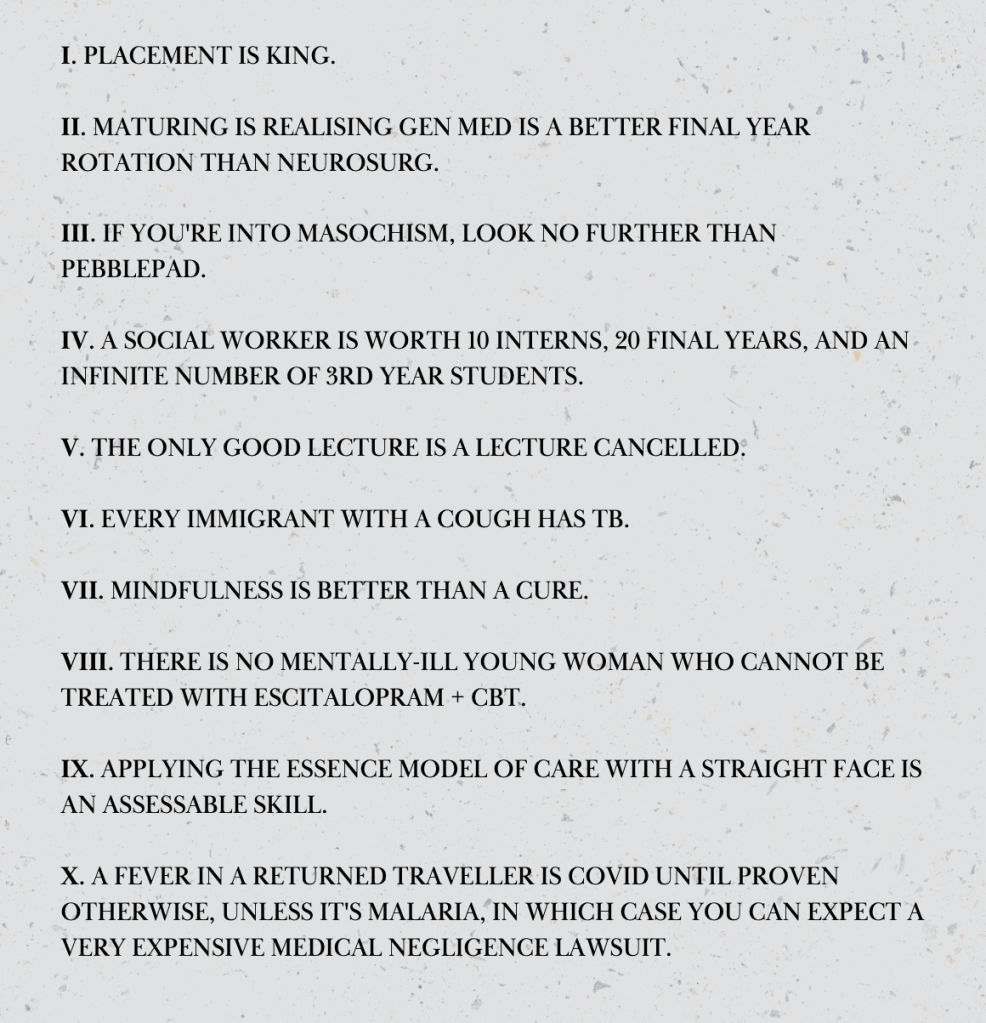
Editor’s note: enjoy this Monash-themed take on the 10 Laws of the House God, from the satirical 1978 novel House of God by Samuel Shem.

Year 5D medical student Dinali Panagodage shares her thoughts on Sandeep Jauhar’s book, chronicling medicine’s understanding of the human heart. This piece was first published in The Auricle’s May-June Edition.

I’m not entirely sure whether this is something that happens to every medical student, but I personally find that as I am reaching the end of my degree, I’m looking everywhere for assurance that a lifelong career in medicine is indeed something to look forward to.
Medical autobiographies are therefore very enlightening. They provide the opportunity for physicians and healthcare workers to share their incredible stories and bring light to the sacrifices this field requires. These autobiographies are certainly holding a strong position on the bookshelves these days, and deservedly so.
Dr Sandeep Jauhar’s Heart: A History opens with Jauhar’s own health scare, the story of which he is all too familiar with: a middle aged man presents with increasing shortness of breath on exertion, who finds out he has significant coronary arterial calcification. Dr Jauhar is a cardiologist and opinion writer for the New York Times, a 9/11 first responder, and the author of three memoirs detailing his experiences throughout his medical career.
This is no ordinary memoir, however. Scattered in-between Dr Jauhar’s stories and own personal experiences, we slowly learn not only about the heart itself, but of the risks and sacrifices that were required to discover the cardiovascular technological advancements that we take for granted today. Jauhar writes in a way where we can see that he’s aware of the delicacy of the subject matter; too much med-ification and the heart becomes nothing more than a glorified pump.
Dr Jauhar takes us through how every discovery and every intervention required someone to ask a difficult clinical question (and sometimes also slightly unhinged: see Werner Forssmann, who developed cardiac catheterisation by doing it to himself). Each chapter begins with a riveting medical story that feels like an action-packed cold opening of a tv show.
“we slowly learn not only about the heart itself, but of the risks and sacrifices that were required to discover … advancements that we take for granted today”
For example, we join Dr Jauhar on Christmas Eve, emergently operating on a patient with infective endocarditis in a quiet but purposeful theatre. It’s in this theatre that we meet the heart-lung machine, and Dr Jauhar takes us on the journey of its invention spanning across decades. Taken back to the 1930s, we learn that the heart-lung machine began with the insane concept of linking one person’s blood supply to another’s (much like a mother and a foetus), and ends with a full-fledged machine that allows surgeons to operate on an arrested heart.
Heart: A History is the kind of memoir that legitimises the journey through medical school, makes you excited to see the discoveries to come, and the possibility to be part of something new. I recommend Dr Sandeep Jauhar’s memoir to anyone fascinated by medical history, and I hope that it captures your heart as much as it did mine.

This piece is the latest instalment in the ‘Spotlight’ series, first published in The Auricle’s May-June Edition. Featuring work from MECCSIG committee members Katie Mazzochi, James Liang, and Jordi Shahab, it takes a deep-dive into the current ambulance ramping crisis.




Samantha Yee is a Year 2A medical student and contributed this moving piece, which was featured in The Auricle’s May-June Edition.
I’ve always thought honesty my shield – that if I have nothing to hide, then there is nothing they can use to hurt me… I know my truth. I stand proud on the challenges I have faced and conquered and revel in the triumphs in my life. Though I am simply traversing the plains of life, equally uncertain and unknowing of the path that lies ahead, my experience might be one others may vicariously extract wisdom from, and I too through theirs.
This is not to say I am to shout out to the world my savings, my social security number: my identity but have I inevitably through the life story I have so willingly shared upon a single question, shared upon curiosity, given up my individuality?
My grandma says getting to know a person is analogous to a flower blooming on a spring day. Its beauty so ephemeral that a rush to bloom will simply hasten the wither. We are but simple creatures: beauty enraptures us, reflections and refractions of light captures our gaze and threatens to never let go – but only for as long as it exists. In our desire to be acknowledged, we forget the evanescence of it all, only questioning thereafter where it all went wrong and how we are left with nothing except the remnants of another’s fleeting attention.
Where do we draw the line between honesty and deceit; self-preservation and cunningness? Why must answers that are given be half-truths? Why should we omit our story for fear that it might be turned upon us and taken advantage of? Why do others seize upon vulnerability and raw emotions and experiences only to mould them into weapons of destruction of the worst kind – the self? Am I to fear that one day, a misplaced trust in another might shatter my shield, leave me defenceless and alone against the prowling wolves of life?
They say I will learn – like a wide-eyed puppy freshly birthed from a mother’s womb, a blank canvas – my elders will be my guide and I shall soon soak up their wisdom to navigate life. But what a paradox that is… because amongst
all the lessons they imparted upon me, they say veiled honesty should also extend to those near and dear – that no one should know me better than myself; that there are secrets of the self that I should take to the grave. What a lonely journey that will be… To be unable to place unconditional trust in the physical is to place unconditional trust in the intangible – life’s most venerated but at times, most unforgiving guide: mistakes.
At this point in time, I am fortunate to still be in the warm embrace of mother life. She is tender and nurturing. Alas, this too is ephemeral. Mistakes of today are tolerated but less certain is this patience for the mistakes of tomorrow and of a few years to come. As we begin to lift from her embrace and onto her shoulders, a fall from this height can be devastating. The gift of recovery is limited and she may only extend it to a privileged select few who she has ascertained has the means to rebound and prosper… I may not be one of them and the ripples of my fall may indirectly hurt those still in her tender embrace.
I may be making a mountain out of a molehill but truth be told, I am fearful. I am questioning the integrity of my shield that took 20 years of life to forge and how difficult it may be to reinforce it and imbue it with newfound mystery. I only ask for the strength and dexterity of an experienced blacksmith to craft my shield to accompany me to the end of this plain.

In this instalment of our Wellbeing Wednesdays series, medical student Hamzah Haggag shares some thoughtful quotations from The School of Life on our approaches to mental health.
“One of the great contributing factors to mental illness is the idea that we should at all costs and at all times be well. We suffer far more than we should because of how long it can take many of us until we allow ourselves to fall properly and usefully ill. In a crisis, our chances of getting better rely to a significant extent on having the right relationship to our illness; an attitude which is relatively unfrightened by our distress, which isn’t overly in love with the idea of seeming at all times ‘normal’, which can allow us to be deranged for a while in order one day to reach a more authentic kind of sanity.”
“It will help us immensely in this quest if the images of mental illness we can draw on at this time do not narrowly imply that our ailment is merely a freakish and pitiable possibility, if we can appeal to images that tease out the universal and dignified themes of our state, so that we do not – on top of everything else – have to fear and hate ourselves for being unwell.”
“The best philosophical background against which to wrestle with mental unwellness would be one that conceived of the human animal as intrinsically rather than accidentally flawed, a philosophy that would resolutely reject the notion that we could ever be perfect and would instead welcome our griefs and our errors, our stumbles and our follies as no less a part of us than our triumphs and our intelligence.”
If we learn to confront our illness without panic or fear…
“We feel less guilty that we are not at work and are not playing up to the roles demanded of us by responsible others. We can be less defensive and frightened, more inclined to seek out proper care – and more likely to recover properly in time. With a philosophy of acceptance in mind, we can recognise that whatever the particularities of our crisis (which will naturally need to be investigated in due course), our pains fit into a broad picture of a crisis-prone human condition. No one is spared. No life can escape significant troubles. Everything is imperfect. We don’t have to know the details of someone’s life to be able to guess at the scale of the difficulties they too will have encountered. We have all been born to inadequate parents, our desires will always exceed reality, we will all make some appalling errors, we will hurt those we love and anger those with power over us, we will be anxious and confused, woeful and lost.
We should accept both that we are profoundly unwell – and that our ailments are entirely normal.”
Quote credits from the School of Life

Enjoy these poignant words on self discovery and improvement by Cindy Zeng from MUMUS Community and Wellbeing as she describes a process of asking important, but sometimes difficult, questions.
The pursuit of perfection is something that runs rife throughout medicine; and with that, comes the inevitable and often obsessive comparison of oneself to others.
You cannot get through (or into) medicine, without being compared to another person, whether that’s through grades, interviews, research, positions or extracurriculars, and this process breeds a group of incredible, successful people who are constantly striving to achieve more.
The desire for self-growth and development is good, but oftentimes it’s all too easy to go down the rabbit hole of comparison.
Question 1: How is everyone better than me at everything?
When I look around at my peers, it’s all too easy to compare myself with someone who’s written ten research papers, or gotten a scholarship I was rejected from, or done way better on exams than me – and it looks like they’ve done it so effortlessly.
This sort of comparison doesn’t only exist within the realms of medicine, it also extends into the rest of life. From the outside looking in, I’m always able to find someone who just seems smarter, more athletic, better at making friends and all around more successful. And this leads to the next question I ask myself.
Question 2: Why am I such a failure?
A term you’ll hear floated around a lot: “imposter syndrome” – you don’t have to look any further than your own cohort to find people who report feeling “inadequate”, “useless”, “incapable” and “out of place”. And I’d be lying if I said that I lucky enough to escape these thoughts.
It’s so easy to write your achievements off as nothing when it seems like people around you are achieving way more and doing it way easier.
Question 3: How do I get better?
This question led to the self-improvement phase, which was just me trying to do everything that I thought a good medical student should do.
I planned my day the night before, woke up early, exercised, meal-prepped, scheduled set times to study, worked hard for long hours, helped make resources and run events for the cohort and – don’t forget work-life balance – I even dabbled in meditation and made time and go out with my friends.
I was doing everything right… yet I was completely and utterly miserable.
Question 4: Why am I so unhappy?
On paper, my work-life balance looked impeccable. I was working towards a version of myself that I’d previously compared myself to and aspired to be. I’d still compare myself to others, but like a disciplined medical student, I’d schedule in steps to adopt their habits and add them to my own routine.
But I started to lose interest in activities that I once loved – exercise became a chore, I was no longer excited about medicine, music didn’t interest me and going out with my friends was just another checkbox on my to-do list.
I used to be such a driven, passionate person who (to the detriment of my productivity) couldn’t resist a chat with a friend or friend-to-be. But now, I felt empty and hopeless, and in the obsessive pursuit of perfection, I felt like I didn’t even know myself anymore.
Question 5: What now?
Being about a year later now, I can’t say that I never have doubts about my abilities, or that I never wish that I could be more like someone else.
But now I do things to enjoy them, not because I think I should be doing them, and I no longer put so much pressure on myself to do the best in everything.
Take it from me when I say that chasing an idealised version of what I thought was the quintessential medical student did not make me happy. Waking up dreading the day ahead and experiencing chronic dissatisfaction surrounding every area of my life was in no way worth the superficial gratification that I got from trying to be impressive on paper.
It took a lot of self-reflection on who I really was as a person, and it took a lot of time to rediscover things that I loved. At times, it felt like I was taking one step forward and sixty steps back, but I can now confidently say that I’m much happier and more confident in who I am as a person.
And instead of asking how everyone is better than me, I’m constantly asking myself:
Question 6: How can I be the happiest version of myself?

In this instalment of our Wellbeing Wednesdays series, Emil Edirisinghe shares some interesting reflections on mindfulness. That often-dismissed practice of meditation can, according to Emil, have a bigger impact thank you think!
We all know that meditation is good for us – we’ve seen the lectures from Craig Hassed, we’ve seen the news segments, we might’ve even seen an inspirational YouTube video about some millionaire who wakes up at 5am everyday to meditate. Much like exercise, reading or eating healthy, we know that building the habit of meditation would be beneficial to our lives, yet many of us (including myself) struggle to do it.
This article isn’t intended to shame those of us who struggle to build these habits – I am certainly one of these people, and that’s OK! Everyone has their own struggles, and managing to eat healthy, exercise, read and meditate is a gargantuan, if not, impossible task (my scarcely used gym membership attests to this). Rather, I want to share my personal experiences with meditation and its positive outcomes in the hope that it can encourage you to try building this habit yourselves. Even if it doesn’t become an infallible part of your routine, I hope that simply trying to incorporate this habit will be a positive experience in itself!
Personally, I have been able to maintain the habit of meditating intermittently for the past 12 months, and I have found that it has offered enormous benefit to my mindset, focus and emotional wellbeing. These words have a relatively intangible meaning by themselves, so I’d like to share some concrete examples of how these benefits have manifested in my life.
Yesterday, I found myself heavily procrastinating on doing some work – I was sitting on my couch, scrolling through TikTok – all students know the drill. If I were to continue procrastinating, I would fall further behind on my work, and feel terrible about myself. Often, we may find ourselves in these situations of mindlessness, scrolling for scrolling sake, for hours on end. Yesterday, however, I had a moment of mindfulness where I actively thought – “What am I doing?” Even though it was brief, it was enough to allow me to make a choice, to stay on the couch, or to get up and do something with my time. In what may be a plot twist, I chose to stay on the couch, but the ability to make this a conscious choice lifted a large burden off my shoulders.
These moments of awareness come more frequently to me as I meditate. Perhaps more impactfully, I find that they also come in moments of intense feeling, such as anger or sadness, but also happiness.
Before meditating, I never had conscious moments of self-awareness when I was angry – I would just be angry. Later on, I might have realised that I had overreacted or been unreasonable, but by that time it would often be too late. Now, the ‘lightbulb’ moment where I can see my own behaviour and say “I’m feeling angry” allows me to understand my emotions in the moment and thus, treat the people around me more fairly. Awareness is also powerful in moments of happiness, where I find myself truly grateful, and thinking to myself “This is really nice”. Rather than feeling mindlessly, I am able to consider my feelings with depth and feel more grounded emotionally no matter what happens.
I’ve found that habits such as exercise and meditation are hard to build as their positive effects are largely long term and intangible. When people discuss meditation, the benefits are to your mood, energy, and focus… In a couple of months! These metrics can be uninspiring and vague, so I hope that by sharing some of the tangible ways in which meditation has benefitted my life, you might be inspired to try it yourself. Even if you don’t try meditation, I hope that this article can help you foster more moments of mindfulness and improve your overall wellbeing.

“It’s always ourself we find in the sea.” These words by e.e. cummings are a beautiful prelude to this weeks’ Wellbeing Wednesdays’ piece by MUMUS C&W’s Faizah Alam. Happy reading!
Over the summer, I made the trip down to Dromana for a short and spontaneous road trip. Therein laid the foundations for my obsession with going to visit blue spaces (be it waterfalls, fountains, oceans or even reservoirs) on every free weekend I could spare. These were preciously guarded trips that I kept constant throughout the first semester this year.
The beach in particular, is one of my favourite places. I get to the beach and I’ve seen it a million times before. Yet some part of me is still imbued with wonder each time at the sheer vastness of what I’m seeing. Most of the time, I go to see a calm sea with waves lapping on shores to leave behind shells, seaweed and little eddies of water trapped in dips of sand. There are however other times when I go to rock formations or cliffs and the controlled violence of the waves hitting rocks is beautiful in its own terror.
I have even found myself voluntarily waking up at 5am to see the sun rise over the shores, and to see that cinematic sunset moment over the full scale around the ocean.
Blue spaces, and in particular, seeing the sea are things that have never failed to reduce my anxiety and stress and just let me be in the moment. With the ebbing flow of waves, it is easy to let go and just not think about the overwhelming responsibilities and tasks that I’ve procrastinated on completing for a while. A systematic review found that there is a positive association between blue spaces and mental health and well-being as well as physical activity. In my own experience, water has always been a way to use all of my senses – sight, smell, hearing, touch and taste – to reduce depression and anxiety. It’s a way to disengage from the constant panic of the world brought on by rushing people around us or even social media and our phones.
It is no wonder that we are drawn to blue spaces as simple as water features or man-made lakes. The small lake adjacent to the Med Building was a favourite lunchtime spot of mine when we were back on campus.
Studies have found that being exposed to oceans, lakes, fountains and other blue spaces may be associated with increased time with family and friends as well as increased social interaction in general. It has been positively linked to hallmarks of social interaction such as a sense of community, belonging and participation. All of these are protective factors and enhance wellbeing and mental health.
Research in this area is in its beginning stages, with the need for more longitudinal research and the distinction of confounding variables required. However, on an individual and personal level, I can’t refute the calming nature that going to these areas has on my wellbeing.

The simplicity in just being and not having or being expected to do anything is what has always drawn me to the ocean and to water in general. To me, it is the perfect description of the ever-changing nature of human emotions. It’s okay to be calm one day then upset and angry the next. It doesn’t make you any less beautiful, any less special and any less in any way.
There is something about the sea that turns us back in time, an implicit need to point it out and just to stop in our tracks with the perspective and wonder about our part in this world.
Studies quoted:

For this fortnight’s Wellbeing Wednesday post, the following artwork was created by Monash student Andy Li.
It’s easy to forget what it’s like to know nothing; to be in the dark about your own body. https://www.abc.net.au/news/2022-05-11/amrita-lanka-monash-childrens-hospital-death/101054286


In The Auricle’s March-April Edition, we share this profile of Ishka De Silva – medical student and President of the Monash Students Association (MSA).



This Is Going to Hurt is poignant and confronting television series which has divided viewers. In this review for The Auricle’s March-April Edition, Co-Editor Jordi Shahab shares his thoughts on the controversial show.

What is the financial burden of having a period in Australia? How does it affect those from disadvantaged communities? This piece lays the groundwork for ending the all-too-common phenomenon of period poverty. From the Women’s Health Interest Society of Monash (WHISM), this piece was written by Palak Gupta, Emily Whalen, Surabhi Shashishekara, and Meghna Prasannan. It was also featured in The Auricle’s March-April Edition.
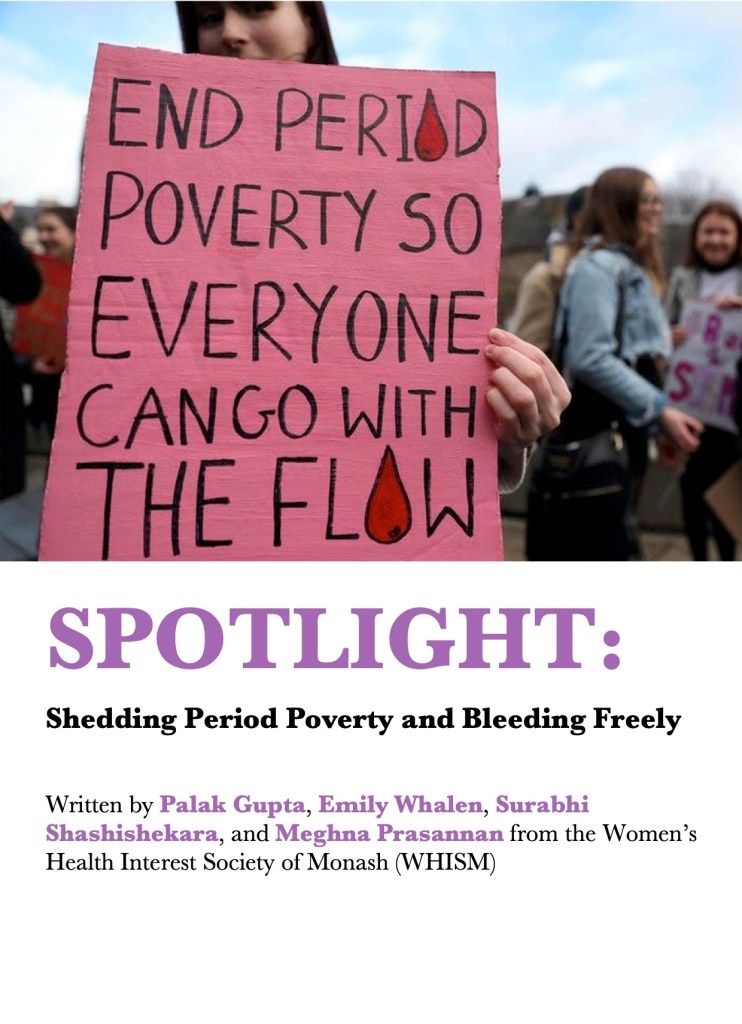
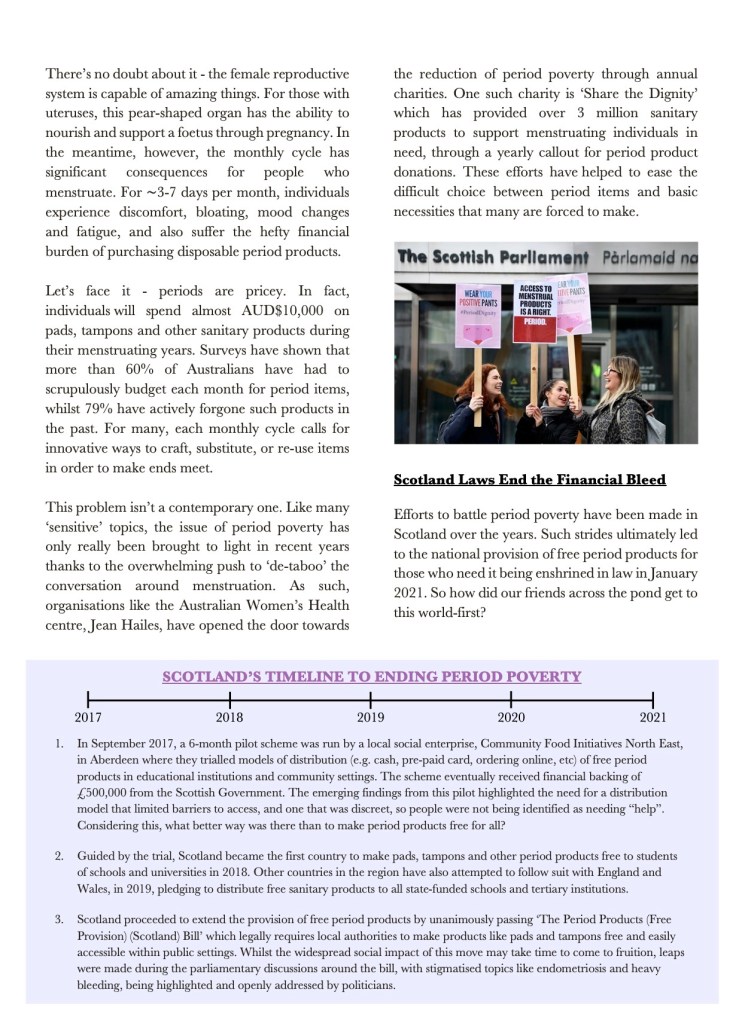


For our regular Research Corner segment in the March-April Edition of The Auricle, Andrew Duan shares his research on Long Covid. An increasing concern as the Covid-19 pandemic rages across Australia, this article is a fascinating insight into an intriguing condition. Andrew Duan is also an Education Officer for the Medical Research Students Society (MRSS).
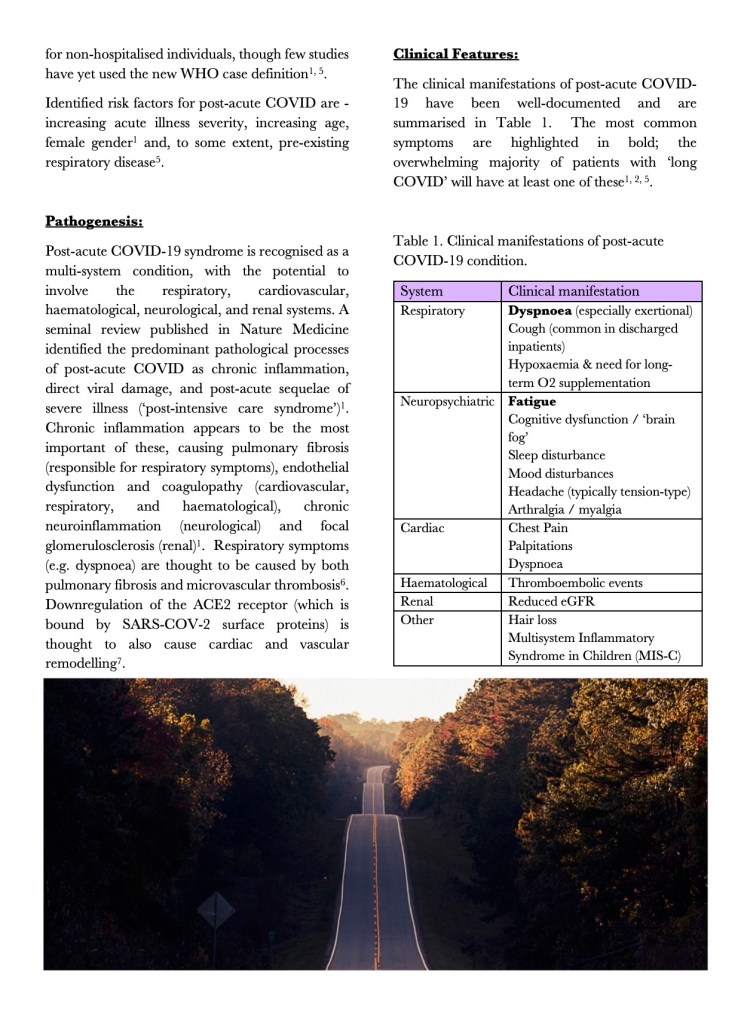


Written by Kylie Choong, the Committee Events Officer for MUMUS Community and Wellbeing, this piece gently articulates the tough isolation that can accompany mental illness, and the welcome relief of connection. This piece was taken from The Auricle’s March-April Edition.

In this beautiful short story, year 3B medical student Devangna Tangri writes from the perspective of a flying friend. Enjoy this wonderful piece from The Auricle’s March-April Edition.

In this poem by second-year medical student Aadhya Vyas, she explains that all-too-familiar feeling of overcommitment – being torn in many directions. This poem was featured in The Auricle’s second Edition this year, March-April 2022, which you can read here.

Welcome to our first instalment in 2022 of the regular segment, Wellbeing Wednesdays. This segment features work from our friends at MUMUS Community and Wellbeing. Today’s piece is from Shreya Mago, who expresses a perhaps familiar feeling of the pressure of self-improvement. Stay tuned for regular updates from C&W throughout the year!
Whether it be being surrounded by inspiring individuals, examples of incredible people in medicine, or general glamorised social media content, medicine seems to breed a sort of obsession for self-improvement and health.
Its the type of self-improvement you read about in self-help books. The one that med students dream of achieving when they obsess over those “day in the life” or “how to increase your productivity” youtube videos. We’ve all done it, no shame or judgement here.
What makes this type of growth so hard is not just the act of having to make that change. Of course, it’s already initially difficult to force yourself to not snooze through that 6am wakeup, hit the gym most days or meal prep on the weekends. But what makes this process of self improvement so much more difficult is our own minds, which seem to criticise us when we stray even slightly from our goal, and can sometimes struggle to accept that improvement isn’t always linear.
Medicine seems to breed a sort of obsession for self-improvement and health.
The 2020 lockdown was a time of self-focus and reflection for many. For me personally, I adopted, what was in my eyes, a healthy routine. I started waking up early, exercising daily, studying at more appropriate and routine times, and caring for my skin properly. But it was a slow process. Some days, I would be tired from forcing myself to wake up early all week and remain in bed for the better part of the day. Which is fine. It takes time for your body to get used to new activities. Only, at the time it didn’t feel fine. I’d be consumed with guilt and anxiety that I’d messed up my routine. After these feelings, there’d be increasing pressure to ‘fix’ things the next day. Do a harder workout, eat healthier, spend less time on my phone. I wouldn’t honour my body’s limits and I wouldn’t accept that adopting habits takes time. It’s not a perfect process, and even when something becomes a habit, it still may not happen every day. I ended up injuring my back and knees through the exercise I was doing, and was essentially told it was because I probably started doing too much, too soon, without giving my body time to adapt.
Even then, I didn’t really process that maybe I was being too harsh on myself. In retrospect, perhaps if I had listened to my body and what was best for it, as opposed to trying to match my life to a perfect, morning routine highlight reel every day, I may not have injured myself.

A couple years later, and I can say that those early wake-ups are now a pretty easy habit for me to stick to, and exercising most days doesn’t feel difficult. And sure, part of it is because it’s been a couple years now and I’m used to it. But even more so, it’s because I no longer put as much pressure on myself. If I sleep in, it’s because my body needs the rest to recover, and I don’t need to wake up feeling as though I’ve already wasted the best part of the day.
Our own minds … can sometimes struggle to accept that self-improvement isn’t always linear.
I regularly see traits or habits in other people which I try to adopt. But I’m realising more and more that I need to go easy on myself. Some days, I’ll get it right. I’ll spend less time on my phone and I’ll read a chapter of a book and go to bed on time. Other days I spend hours mindlessly scrolling on my phone and not getting enough sleep. But this is also fine. It’s a process of learning, and feelings of guilt only hinder our ability to function.
I can’t say that I no longer feel that guilt or anxiety, but I’m getting better at managing it. And I urge anyone who has felt this way to recognise that when you try to learn or improve yourself, ultimately you’re doing it for yourself. So why strain ourselves with harsh criticisms of everything that didn’t go perfect, and instead take things as a learning opportunity. Appreciate what went well in the day, what you achieved and what made you happy. And when considering what you could have done differently, rather than feeling that you’ve messed it all up, recognise that it’s a process, and when you get it, you’ll get it, and if you don’t today, that’s fine too.
Shreya Mago is the 2022 Co-Chair of MUMUS Community and Wellbeing

Welcome to the Spotlight segment, new to The Auricle in 2022. In this featured article from our January-February Edition, Co-Editor Lachlan Coman tells the tale of one of the rarest blood groups in the world.



Ben Hunt is a keen photographer, with a particular focus on the natural world. In this photo journal, Ben explores the volcanic geography of the Mornington Peninsula.
Featured above and below are just two of his photographs, “Elephant Cliffs” and “Gunamatta Dragon”. To see the rest of Ben’s photos, and read his words about the creative process behind them, follow this link to the January-February Edition of The Auricle where you can see them in high definition.


2022 Co-Chair of Community and Wellbeing, Virginia Su, shares her artistic reflections on living in the moment. This piece was featured in The Auricle‘s January-February Edition.

Featured in our January-February Edition, this poem is by talented Year 3B student Savannah Mandakini and compellingly describes the common struggles of deadlines, procrastination, and that feeling of falling behind.

For our January-February Edition, Co-Editor Jordi Shahab spoke to medical student and lifeguard Izzy Greer.
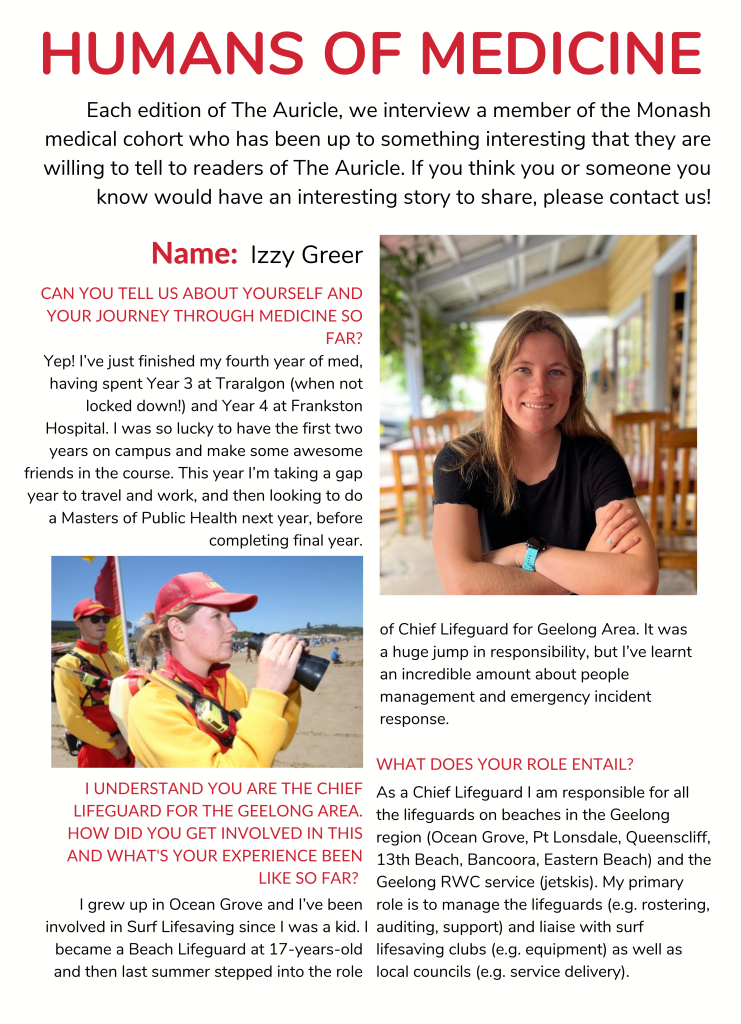
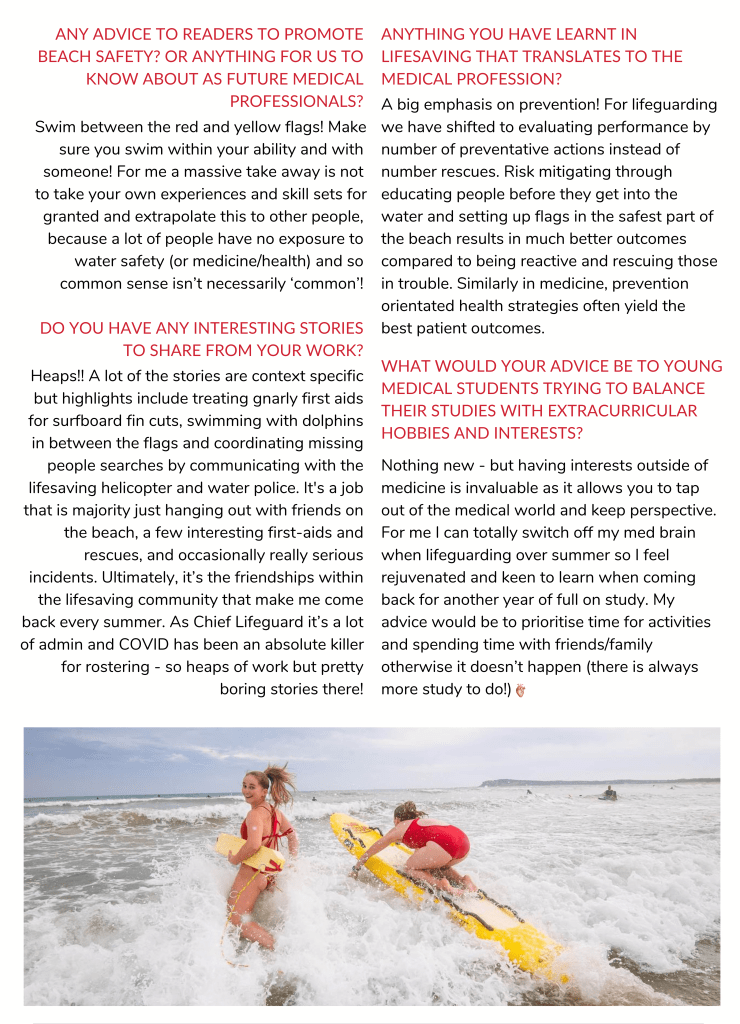

Each Edition, our wordsmith-in-residence creates a tantalising brain teaser for you. Take a look at the crossword from our January-February Edition, where you can also find the answers!

Jasmine Elliott writes of the much-loved, and much-missed, John Flynn Placement Program. Featured in our January-February Edition, this piece describes how the program came to a sad end.


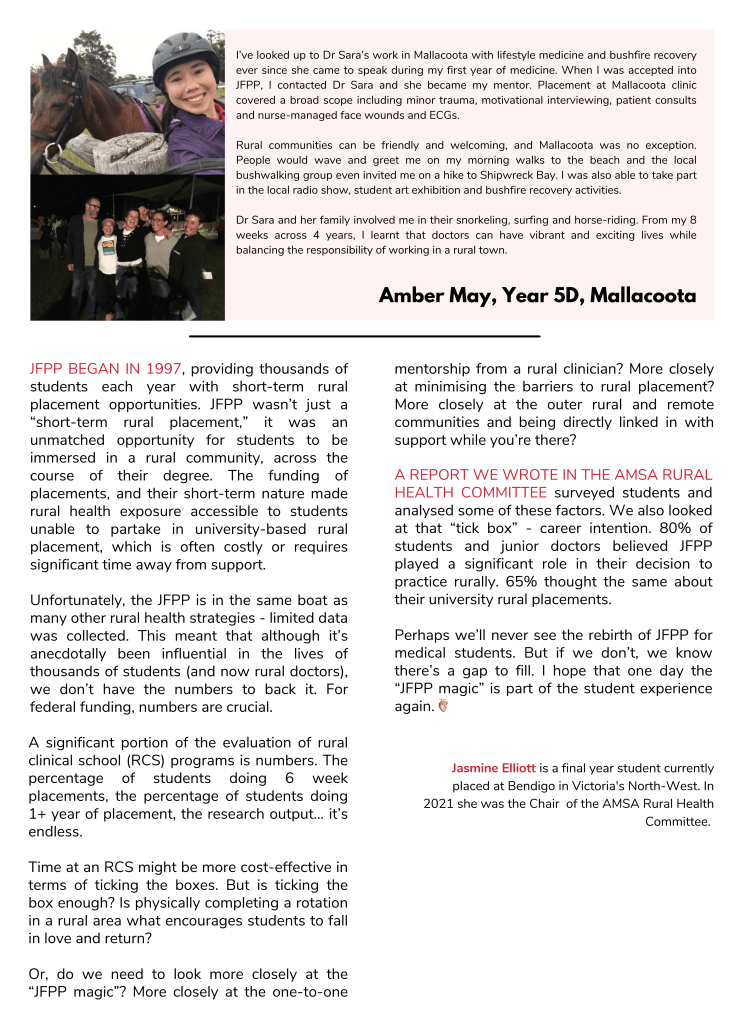

Welcome to a new segment in 2022 where Monash medical students can display some of the research projects that they have been involved in. Our first instalment from our January-February Edition features Vikash Yogaraj who writes on the relationship between thyroid disease and symptomatology.
We hope you enjoy, and stay tuned for more research to come!
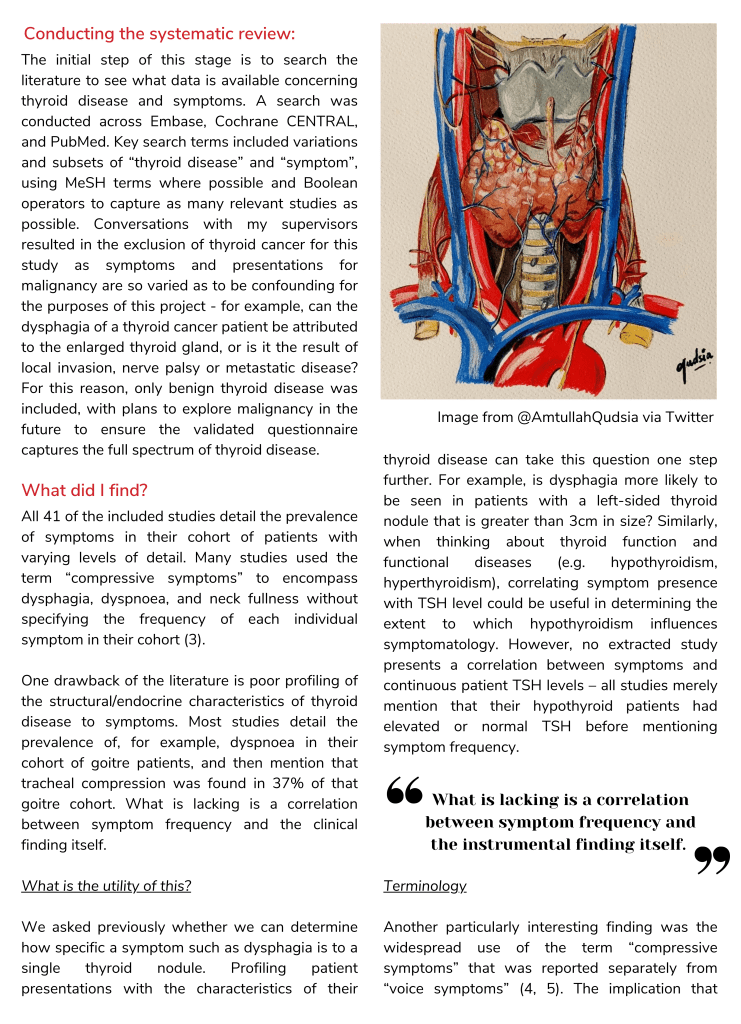


The 2021 AMSA National Leadership Development Seminar, though held online, greatly influenced and presented essential personal and professional skills for medical students. Here are the reflections of three Monash students, sharing their experiences of the event and tips they received from the speakers they heard.


Despite being held online, NLDS 2021 was truly an eye-opening experience! It was an incredible privilege to hear from doctors and leaders involved in leading Australia’s response for COVID-19, all of whom are inspiring examples of great science communicators. From learning about the importance of creating a self-narrative, to hearing A/Prof Melissa Kang talk about her insights as a medical consultant behind the ‘Dolly Doctor’ column, and learning about the intersection between legislation and medicine, these insights have undoubtedly enriched my thinking. In addition, keynotes from experts allowed me to gain valuable insights about how they overcame challenges to achieve success in their extraordinary career trajectories. Furthermore, practical skills on how to approach a problem as a leader, how to write more compelling applications, ways to approach a mentorship opportunity, and how to prepare for an important meeting are also some of my key takeaways from NLDS 2021. All in all, my experience at NLDS has definitely widened my horizons to the vast possibilities of leadership within the field of medicine. NLDS not only showcased inspiring examples of advocacy by doctors, but also allowed me to reflect on my personal leadership goals and gain skills that would make me a better doctor in future!

Being at a conference about the role and importance of leadership in medicine, I must admit I was taken aback when Dr. Vijay Roach, president of the RANZCOG, said this in his talk. As he went on to unfold the importance of humility and the keys to effective communication, I realized that most talks that weekend had subverted my expectations in an exceptionally unique way – every distinct story the speakers told conveyed such meaningful and applicable lessons that made me reflect on my life thus far and prepare for the future ahead.
It was a privilege to hear from the current leaders of the medical field in Australia: people who’ve not only shifted paradigms but are also willing to set forth their failures, positions they’ve been rejected from, and how those key moments shaped their journey. From Professor Peter Doherty discussing the pandemic and its end to Dr. Jessica Dean talking about challenges in advocacy, to individualized project pitching masterclasses with Dr Renee Lim, each speaker highlighted the myriad of possibilities ahead.
I assumed shifting to a virtual conference would mean forgoing the social aspects of NLDS but once again, expectations subverted. All the delegates formed such an insightful and lively group of people who kept engagement at an all-time high – it was such a pleasure meeting everyone and forming lasting friendships.
The team at NLDS21 somehow managed to crack the code for subverting zoom fatigue in the day, and creatively crafting stellar social events in the night.
The 2021 AMSA National Leadership Development Seminar, though held online, greatly influenced and presented essential personal and professional skills for medical students. Here are the reflections of three Monash students, sharing their experiences of the event and tips they received from the speakers they heard.

In an era of Zoom fatigue, NLDS was the one webinar that had me actively engaged and sitting on the edge of my seat. And that’s saying a lot, when I struggle with any class longer than one hour!
It is such a privilege to have had the opportunity to listen to the unique experiences of the speakers and learnt some key lessons to bring into my personal and professional life. As a quieter individual, I have struggled with the conventional idea of advocacy requiring the loudest person in the room. Instead, advocacy is about exploring who needs to listen and how to shape your thoughts in a way that directly impacts them.
The project, despite being optional, is something I would thoroughly encourage any future delegates to take up. It was truly one of the wildest 48 hours I have ever experienced, and certainly not devoid of the panic and cramming of university group assignments. However, the opportunity to work with such passionate individuals who were determined to make a tangible project with such potential and have it evaluated for implementation by prestigious AMSA figures was an opportunity like no other. Big shoutout to Nebula and Jas ❤

If there’s one take-away from any leadership seminar, it is usually to fall down seven times and stand up eight. NLDS 2021 certainly demonstrated this in its inaugural online format, which made for a flexible and engaging event with a variety of high-profile guest speakers despite lockdown. So what exactly can a first year medical student (with an abominable wifi connection) take away from a virtual NLDS? Here are the 3 tips I picked up… and the personal interpretations that I’m taking with me.
Tip #1: Be open to new opportunities
Translation: The ‘doctor’ is a fluid character and every student that enters the med school conveyor belt leaves with unique experiences. Our workload might feel overwhelming and it can be difficult when we are sizing ourselves up against practitioners who have national certifications in their co-curriculars, have published more journals than there are bones in the foot, or successfully balance fully fledged families with their irregular ED calls. However, we all have 24 hours in a day, and apart from the time consumed by our uni timetable, we have liberty over what is scheduled in between. Pick up a new project – it can be unrelated to Med! Read a different genre. Listen to a rising artist. These are the small opportunities that might just help us find the niches that we end up pursuing beyond the ‘hobby’ status.
Tip #2: Operate with restraint
Translation: Establish your principles and limits. What is it that we value most and why are we studying medicine? Every student, like every doctor, must find the courage to say what they agree and disagree with doing. One day, we could be the case studies in an ethical dilemma, and it will boil down to our personal values and reasons for working in the field, in the first place. We can begin by signposting in our own lives, leaving ourselves hints for future reference, for when the current time becomes the past memories and experiences that we look back upon. Ultimately, we need to learn to follow the advice that we give to others.
Tip #3: Lead for the 80%
Translation: The percentage sign might immediately draw our minds to assessment tasks and exams, but this 80% is actually in relation to the people around us. Despite our best efforts and intentions, medicine does not lend itself kindly to unorthodox ideas, and as future doctors, we have to keep in mind that reshaping the healthcare bubble is more work than an individual can achieve on their own. While this possibly means that we will not be able to do enough for 10% of the population in our own time, and another 10% of patients will believe that we are intervening beyond necessity, there remains an 80% whom we will lead, and that our medical advice will have a visible impact on. There is no need to wait for someone to create change, when we are the ‘somebodies’ who can do so of our own accord, from day one.
Now, if there’s one take-away from any first year medical student’s writing piece, it is usually that Zoom is not the ideal place to begin the pre-clinical journey, let alone attend the NLDS. Despite this, I am confident in saying that the artistic licence that results directly from a combination of poor bandwidth, choppy shared screens and buffering audio, leaves me with the above (hopefully creative) translations, from what otherwise would probably have been three very profound and professional tips.
In all seriousness, let’s find ways to incorporate new opportunities into our lives, remembering to operate with restraint and lead for the 80% (at least). NLDS 2021 was a pleasure to attend, and is certainly an event I would encourage students to keep an eye out for in coming years.

As Jane Austen writes in “Persuasion”, “we each begin with a little bias and upon that bias build every circumstance in favour it”. Each one of us navigates the world differently, picking up a multitude of experiences which shape our values and views of what surrounds us. ‘Crossing the aisle’ is an understanding that, inherently, we see things differently. It’s about meeting others where they are at. Paying attention to what their values and views are and using this to build common ground and a shared vision that is in everyone’s best interests. Rather than claiming your view as ‘the truth’, taking time to understand opposing views and facilitating two-way discussion without judgement or confrontation.
NLDS taught me the art of advocacy and the importance of not simply raising awareness of an issue that exists, but more importantly coming equipped with solutions that can be explored. It taught me that there are many more stakeholders within an issue than we think and to carefully consider the impact of changes on all stakeholders involved. Taking the time to learn more about what is valued by other stakeholders and having a strong foundation of your own core values is a fundamental skill in crossing the aisle in leadership and is one that I hope to encompass as a future doctor.
Legend for you
Blue dots signify innocent lives
Red mostly for trauma and blood shed
Yellow for the opportunities and resources we have
Green for glimpses of hope and growth
And the rest is up to you
It’s not hard to understand
It’s easy to stay oblivious, look away
It’s difficult though
For me
And for the rest of us
Who have had to live the experience
Who have had to do nothing but just watch
And quite frankly
Times I have had to look away
To preserve what I have left
When there is so much to see
I’m aware some of us have lost our sights
Either against our will or through our actions
But I promise you I still see things
And that I will make sure I do
And that the rest of the lenses do
We will see this through
Yet for now, choose your battles
We want progress
We rest.
For more information on Myanmar and how you can provide support, please visit the following links.
Mental Health Support Services
